

As you may remember, I have been helping Dr. DePasquale develop her theory concerning the need for differentiation between hospital mergers and system-joiners. Because Dr. DePasquale coined the term “system-joiner” herself, she is soon putting out a new paper that elaborates on what exactly this specific type of consolidation looks like. Dr. DePasquale argues that within the realm of health system consolidation, a system joiner allows the joined health system to exercise monopsony power.
What is a Monopsony?
Even if you don’t study economics, you’ve probably at least heard of a monopoly, an economic system in which only one supplier of a good or service exists, and where the occurrence of unfair competition is highly likely. A monopsony is analogous to a monopoly, in that only one buyer of a good or service exists. Such a scenario is most often associated with a monopsonist employer that demands the labor of multiple workers.
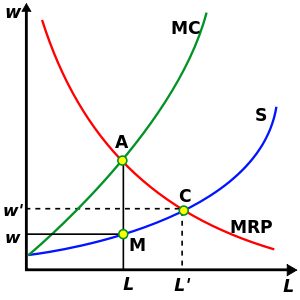 We can look at the above graph to see how monopsony power is exercised. In a competitive market with multiple employers and multiple workers, the level of employment and wage would be determined by the supply and demand equilibrium, seen in the graph as L’ and w’. However, because in this case the monopsony is the only employer, the monopsony can maximize its revenue by choosing the level of employment consistent with where marginal cost is equal to marginal revenue, while also minimizing costs by setting the wage w equal to where our level of employment L intersects the supply curve. Thus, this monopsony is acting in an anticompetitive manner because it can lower wages so that they are less than its marginal revenue while still retaining a profit maximizing level of employment.
We can look at the above graph to see how monopsony power is exercised. In a competitive market with multiple employers and multiple workers, the level of employment and wage would be determined by the supply and demand equilibrium, seen in the graph as L’ and w’. However, because in this case the monopsony is the only employer, the monopsony can maximize its revenue by choosing the level of employment consistent with where marginal cost is equal to marginal revenue, while also minimizing costs by setting the wage w equal to where our level of employment L intersects the supply curve. Thus, this monopsony is acting in an anticompetitive manner because it can lower wages so that they are less than its marginal revenue while still retaining a profit maximizing level of employment.
What Does Dr. DePasquale’s Research Show?
While in theory the monopsony is a well known market structure, there is little to no empirical research that shows evidence of monopsony power taking place. Dr. DePasquale’s research could be the first of its kind to provide findings supporting the existence of a real life monopsony. Her paper examines situations in which one or more local hospitals are absorbed into a larger regional health system. After the consolidation takes place, only one major health employer remains. Dr. DePasquale found that this transformation allowed the system to lower wages across the board while simultaneously retaining a similar number of employees. This suggests that that the consolidation allowed for a monopsony to emerge.
What am I Doing to Help?
After presenting her paper for other economists to critique, Dr. DePasquale was confronted with a number of new questions regarding her research. The most recurring question seemed to be: “How do you not know that the hospitals are substituting their current employees with less skilled workers to justify the lowering of wages?” i.e. replacing a nurse practitioner with a register nurse, replacing a physical worker with technology, replacing an American citizen with a foreign nurse, etc. Expanding on this question, some other economists said if the same thing could be true at the physician level. However, this drew notice to the fact that Dr. DePasquale was unable to find hardly any substantial data on the number of physicians by hospital or by market, as well as any information alluding to the wages of said physicians. I will be tackling both of these issues, so that the paper can be sent out with a more believable finding of a real life monopsony.