The topic of death and dying is something I’ve researched before and take great interest in. The topic of death is so complex and mentally draining that talking about it makes me go through emotions. Last year, I took a course on this topic and gained much newfound knowledge, specifically regarding the dying process. In a way, death and grief are a cycle that we all experience, and this pandemic highlighted that.
As COVID has gone on, we have become desensitized to death. Every life has become a statistic, with countries being in a pseudo-composition for who has the highest number of deaths. I think that the HIV/AIDS epidemic differs from COVID-19 in that people have less incentive to know the deaths and impact of the disease; specifically, with CIVID, anyone and everyone can become infected. With HIV/AIDS, only those who are exposed to it through sexual activity really focused and cared about the numbers and deaths.
I think a significant component of death is within the time range. Those with a life-ending diagnosis will have to grieve for a stretched-out period compared to someone who dies from an illness within minutes or days. Those who have to grieve for an extended period tend to go through (and possibly complete) the cycle of grief, which in itself is torture. Accepting that you are dying is not an easy pill to swallow. But in the end, we all technically know we will die. It creates the philosophical question, “If I’m going to die regardless, how does a life-ending diagnosis make me grieve my death more?” “Is it better to know when you’ll die or have it happen at any moment without knowledge?”
During week 10, Dr. Raper really sat down with the class and unpacked mental health, and reached into those taboo topics. One topic we covered that stood out to me was the idea of helplessness.
I will say that the feeling of helplessness is the feeling I loathe the most. Helplessness is something I definitely felt during the pandemic. Coming from an immigrant family and being the eldest child & daughter, the responsibility of being a parent for my siblings fell on me pretty early in life. I used school and extracurriculars as a way to be independent and free. However, when this was taken away from me during the pandemic, that feeling of helplessness set on me. In a way, that helplessness turned into dependency, which again is something I despise for myself. Discussing the feeling of helplessness during class made me tap into that period of my life again, and I found myself feeling those same feelings during the lecture.
Mental health is such a taboo topic, especially in the Somali community that I come from. Like me, many people try to get help for mental health outside their communities because their own community will dismiss their concerns or invalidate them. I remember feeling extremely helpless and borderline depressed when I discovered my graduation was canceled. I voiced these concerns to my mother, but they were dismissed, and I was told to be grateful that I was alive while many others were dying. To me, that was soul-crushing, mainly because I am first-generation, and graduating high school would’ve been a significant accomplishment. For mental health to become a stigma is terrifying because we all experience times when things get rough or might need a little help. I hope that in the future, if we are put into another situation where we need to lock down (hopefully we don’t, knock on wood), mental health will become less of a taboo and that people will receive the support they deserve.
During Week 9, we had the Emory Outbreak Response Team and Dr. Melanie Thompson present on community engagement during the COVID-19 pandemic. I believe that without public engagement and awareness of the COVID-19 Pandemic and HIV/AIDs Epidemic, we would not have been as successful as we are today.
With HIV/AIDS, the importance of education and prevention through affected communities made it possible to slow down the spread. Communicating with the public through commercials, videos, social media, newsletters, and other forms of media made knowledge much more accessible; this is done through community engagement. I feel like this generation is much more open to discussing topics deemed as ‘taboo,’ such as sex and STIs/STDs, which has been the most influential thing. The first time I heard and learned about HIV/AIDs was seeing a safe-sex condom commercial warning about HIV by Charlie Sheen. I remember googling what HIV/AIDS was, but still confused, I asked my mother what it was. This promoted a long conversation between us where I was told lots of misinformation. Even though pubic engagement is a tremendous positive for providing knowledge and spreading information, it is also a double-edged sword.
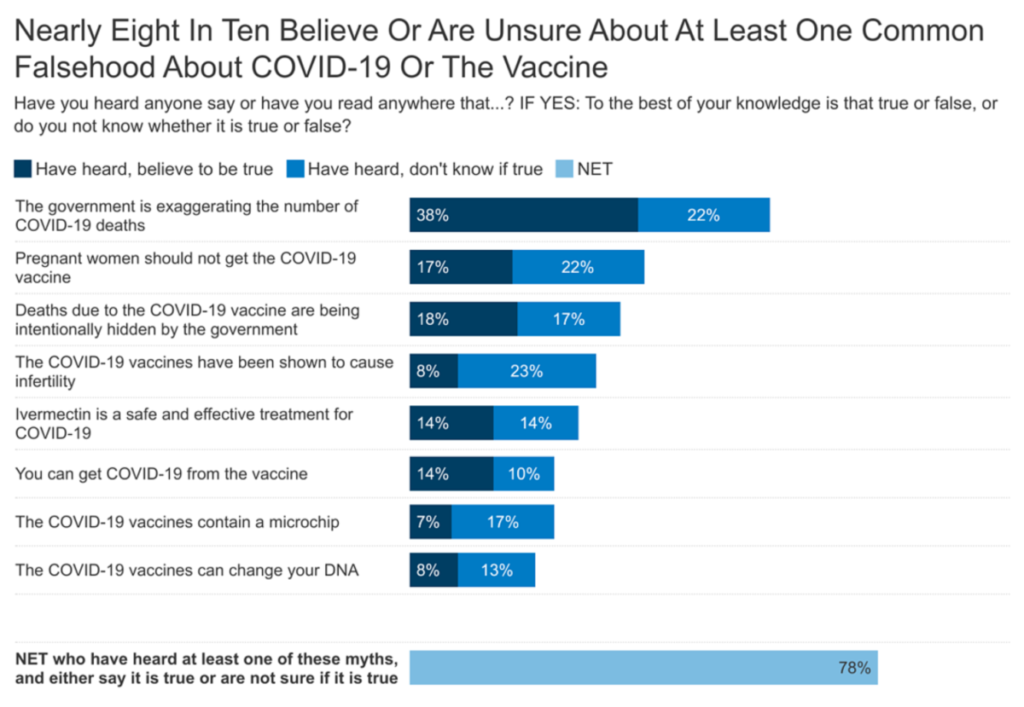
The spread of misinformation can be detrimental to communities because it significantly influences how communities engage and react. With HIV/AIDS, misinformation containing homophobia, racism, and incorrect information has debilitated those affected and has made the topic more taboo. With COVID-19, misinformation spread through the community through public figures, specialists, and other influencers have made the public uncertain or believe misinformation about the pandemic, causing more deaths and illnesses.
During COVID-19, so many myths and misinformation were spread that most people believed something incorrect. I remember hearing conspiracy theories about the vaccine, such as it having chips put in by the government, the vaccine itself giving someone COVID, the vaccine as a form of population control, etc. Some are definitely more ridiculous than others, but with the help of people who debunk the myths and provide accurate facts and data, their ability to spread this info was successful. Through partnership and public engagement, the death and infection rates have decreased, and society has had the ability to shift to an in-person world.
In last week’s lecture, we had multiple speakers from Emory’s community come out and discuss the impact of COVID-19 on education. One aspect that stood out to me, and I have grown passionate about these past couple of years, is disability resources for students, specifically comparing remote settings and in-person settings. The mental health resources provided to students during regular school years are not great. Emory is no different. Emory’s central mental health resource is Counseling and Psychological Services (CAPS). Even though CAPS switched to a remote telehealth form during COVID-19, only those who were still residing in Georgia could receive services. Thus, many people who were forced to go home did not have access to CAPS.
Before COVID-19 and even now post-COVID-19 (are we really post-COVID-19, though?), CAPS was severely underfunded and lacked proper staffing to meet the needs of students. Mental health has always been something Emory students have struggled with. According to the website Humans of University, they placed Emory at no. 4 for the most depressed student body. Whether that is true or not, one thing I know for sure is that Emory’s mental health resources are inadequate to help all struggling students. I’ve had personal experiences with CAPS that, unfortunately, seem to be universal.
When I first signed up for CAPS, it took a few weeks to have an initial meeting to determine my needs and intake. When I was asked if I had preferences, I requested to be assigned a therapist who is a person of color or a woman simply because I believed that these criteria were important aspects of my life that would be better understood by someone who can relate to me. This caused me to experience a wait time of 3 months, which was absolutely ridiculous. The average wait time for CAPS is about 2 months, but because I had preferences (which aren’t extremely picky or detailed), I was forced to wait an extra month. That is not a reasonable wait time for students reaching out for help. On top of that, it should not be difficult to provide students with a woman therapist or a person of color; Emory has thousands of students who identify with those identities. The staff should also reflect that.
Figure 1 Source: National Alliance on Mental Illness (NAMI)
Mental health is not the only form of disability that exists, of course. During COVID-19, certain students with physical disabilities, including myself, struggled with remote learning. I have visual impairments, and so being on Zoom and on my computer for hours on end brought me so much eye strain and pain. Many students with various physical disabilities struggle to do remote schooling because physical schools provide specialized learning and tools to help those disabilities. For many parents in the country, it forced them to become teachers for their children with disabilities so that they did not fall behind. However, according to The Washington Post, parents with children that receive special education “… are not just falling behind academically but are missing developmental milestones and losing key skills necessary for an independent life.” The pandemic was a really rough time for disabled students, and there weren’t many resources provided to relieve students.
Emory’s main resource for disabled students is the Department of Accessibility Services (DAS). While DAS could not provide much help during remote learning, just like CAPS, it is severely understaffed and underfunded. There is too much demand from students and insufficient staff members within the department. I’ve also been personally affected by this; I applied for accommodations at the beginning of this semester and, 3 months later, have yet to hear anything. At this rate, the semester is nearing its end, so what would DAS be able to do for me? It’s truly a shame.
Figure 2 Source: American Medical Student Association (AMSA)
For a university that costs nearly $80,000 a year, you would think that vital departments, such as CAPS and DAS, would be properly funded and staffed. Unfortunately, this pandemic has shown us that this is not true, and their limitations are extensive. Hopefully, enough awareness and conversations with the administration will improve things and implement change.
On October 4th, a professor and author named Dr. Steven Thrasher visited our class on his new book tour, The Viral Underclass. His work focuses on different health crises, such as the HIV/AIDS epidemic and the COVID-19 pandemic, to explain how viral underclasses are constructed, Thrasher presents that 12 vectors contribute to this creation: racism, individualized shame, capitalism, the law, austerity, borders, the liberal carceral state, unequal prophylaxis, ableism, speciesism, the myth of white immunity, and collective punishment. Personally, I was quite intrigued about how racism and capitalism (specifically with mass incarceration) play out depending on the health crisis and how they are interlinked. Therefore, I’ve realized that comparing these two vectors will help us understand how history basically repeats itself.
HIV/AIDS
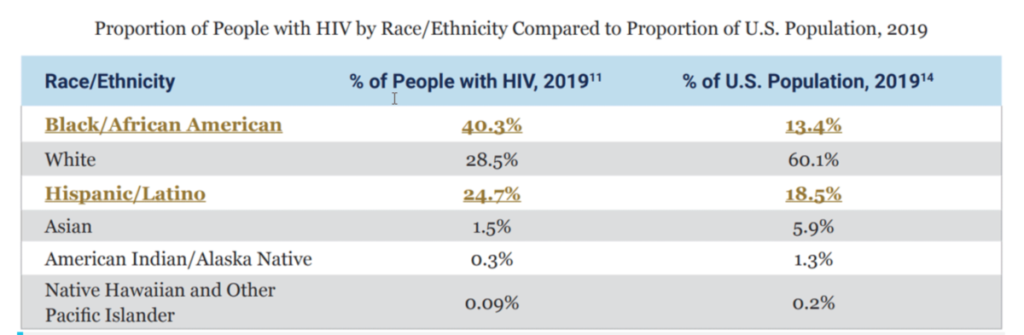
With the HIV/AIDS epidemic, the communities that are the most disproportionately affected are Blacks and Lantix/Hispanics. In these communities, adequate treatment, prevention, and education are not reaching these groups, even though they are the most impacted. Racial discrimination, stigmas, and class status, all influenced by history, are a few factors that have allowed this disproportion to occur. The table below compares the percentage of people within racial groups that have HIV compared to the total population percentage within the US.
Figure 1 Source: CDC
Black/African Americans and Hispanic Latinx people are the two racial categories whose total population percentage with HIV exceeds their total population percentage within the US; this emphasizes how these groups disproportionately experience inequity and inequality due to race during this epidemic.
Another factor that promotes inequity with HIV/AIDS is the capitalistic system that established mass incarceration. Mass incarceration is essentially modern slavery; when the Crack Epidemic occurred in the 80s, most low-income, poor Black communities fell victim to the epidemic and struggled with drug addictions. When the US implemented the “War on Drugs,” the US government heavily targeted Black communities and created laws that targeted these communities and created inequities. One great example of this is the crack vs. powder cocaine disparity which has a 100:1 quantity ratio. Since prisons are private entities, they have practically become businesses that need more prison beds filled to receive more money. Prisons are free labor without any rights, and essentially, the way the system is set up makes them ‘socially dead’ (i.e., unable to partake in society, such as voting, getting jobs, etc.). The author Ruth Wilson Gilmore pinned the term “Golden Gulag” in her book Golden Gulag: Prisons, Surplus, Crisis, and Opposition in Globalizing California to describe the current mass incarceration epidemic within California and further explain how mass incarceration is modern slavery.
According to HIV.gov, they state that “The rate of HIV among prisoners is 5 to 7 times that of the general population. HIV rates are highest among black prisoners. The correctional setting is often the first place incarcerated men and women are diagnosed with HIV and provided treatment.” They also explain that although these incarcerated Black and Hispanic/Latinx communities are at high risk for contracting HIV, most prison facilities haven’t implemented prevention, testing, and treatment options for inmates (HIV.gov). When inmates contract HIV, they might be isolated and prohibited from participating in prison-sponsored activities. Sometimes, their HIV status is not also private and is disclosed to others, promoting discrimination and stigmas to those affected.
With the COVID-19 pandemic, similar experiences and practices within the HIV/AIDS epidemic are seen occurring with this pandemic. In terms of prisoners and those trapped within mass incarceration, they were ignored. Prisoners during the COVID-19 pandemic accounted for extensive infection rates and outbreaks within the country compared to those not incarcerated; yet, those incarcerated had the fewest vaccination rates. In a journal posted by The Lancet, they explain that “According to the COVID Prison Project, state prisons have over three times the rate of COVID-19 infections than the general population, and most of the largest COVID-19 outbreaks in a single site in the USA have been in prisons and jails.’ As discussed with the HIV/Aids epidemic, many of those that are incarcerated are Black/African Americans. Outside of prisons, though, the Black community was still disproportionately affected by COVID-19 more than any other group.
COVID-19
In Black communities, mortality and complication rates within the COVID-19 pandemic have skyrocketed—lack of access to vaccination sites, misinformation and lack of education, and lack of resources/health care are all various components that are influenced by racial division and racism (historically and currently). Data collected from Maritza Vasquez Reyes in their research, “The Disproportional Impact of COVID-19 on African Americans,” explains that “Approximately 97.9 out of every 100,000 African Americans have died from COVID-19, a mortality rate that is a third higher than that for Latinos (64.7 per 100,000), and more than double than that for whites (46.6 per 100,000) and Asians (40.4 per 100,000). Just like HIV/AIDS, the group that needs support and aid the most is the group that receives the least. More data provided by the CDC in Figure 2 help illustrate how disproportionately COVID-19 impacts Black/African-Americans.
Figure 2 “The proportion of deaths from coronavirus 2019 (COVID-19) in African Americans versus proportion of African Americans in state population, from states reporting preliminary data. COVID-19 data are from the COVID Tracking Project [16], and state population demographic data from the US Census.” Website: Pubmed.gov
Opinion
I personally believe that Dr. Thrasher’s 12 vectors are all interconnected, with some even co-dependent. Whether it’s COVID-19, HIV/AIDS, or any other health crisis, without fail, inequities are brought to light and remind us that there is so much more work needed to be done than simply just finding a solution to the health problem. Inequities are a pandemic themselves. Focusing on the United States alone, our history of slavery, discrimination, xenophobia, sexism, and homophobia still plays out today and affects the lives of millions. Whether it’s through a pandemic or hate crimes, these inequities will never be resolved without proper recognition and active improvement on a local, state, and federal level. We need proper funding for these affected communities, educational resources, and basic access to health care. The current legal system, the law of the land, affects everyone single person but yet promotes so much inequality and inequity. We all should understand that to receive equality and justice for all, equity is necessary and makes such a difference.