“We are each other’s harvest/We are each other’s business/We are each other’s magnitude of bond.” – Gwendolyn Brooks.
When Dr. Stephen Thrasher mentioned the two separate people who shared this poem excerpt with him after reading his book The Viral Underclass, I felt so much of my interest in infectious disease click into place.
Being as intensely interested in viruses and infectious disease as I have been for as long as I can remember has often felt more macabre than uplifting, but hearing Dr. Thrasher describe how viruses exist in the brief spaces of connection between us made me feel something that I am finding difficulty in explaining. Perhaps it was a sense of belonging? I truly felt that Dr. Thrasher put the reason behind my interests into the words that I could never find. I find the way that humans interact with each other and with the world around them to be intensely interesting, and viruses are the byproduct of those interactions.
Humans are social creatures. We thrive in communities, in family units, and with those that we care about surrounding us. The idea of a minuscule, invisible to the naked eye, single-celled organism being able to threaten one of the tenants of our species is fascinating, in theory. In practice, deaths from COVID-19 were not only from the virus–the United States experienced the highest ever combined rates of death due to alcohol, drugs, and suicide during the COVID pandemic. As with the virus, however, those deaths disproportionately affected a certain group of people more than any other: the same group of people who are named as The Viral Underclass. These deaths disproportionately affected poor, people of color.
Within the United States, racism rears its head in an innumerable amount of places. It seems that most issues currently afflicting our society are either caused or worsened by racism. As Dr. Thrasher discussed within his 12 vectors, and as we have seen through our studies of both COVID and AIDS, racism cannot be ignored whatsoever in the world of public health. Yet, many people–even senators–do their best to argue that racism no longer exists within the United States.
In my opinion, one of the reasons for the increasing politicization of public health is the way that it seems to be intrinsically intwined with leftist thought. How can one examine any public health issues without understanding the United States’ ever-going attacks on Black bodies? How can someone look at the amount of acute and chronic infections that disproportionately affect people who have/are experiencing incarceration and not believe that there must be a better system possible?
We are each other’s harvest, business, and magnitude of bond. We must take care of one another, no matter how hard viruses–or any other factors–may make it.
Dr. Musa Dube unique story-telling mode of communication shed light on previous lecturers’ message on the effects of choosing the “best” messenger. In her story, the best messengers that united the people to take initiatives against COVID19 were not necessarily the one who knew the most about the virus but rather the one who spoke in a discourse understood by the community – the religious discourse. Such an approach to communication resonated best with the people to whom they spoke – not because it provided indisputable data nor laid out rigorous reasoning. Importantly, it drew from this “trust” reservoir of the community, nurtured by their belief in the same religion. We can see a similar effect during the HIV/AIDS pandemic, when Magic Johnson announced his HIV diagnosis. The reason people believed the dangers of HIV/AIDs when hearing his announcement wasn’t because he pulled up a physician-approved medical report but rather it’s because he is known to love, and be really good, at basketball, yet is now making the drastic move of retiring following this announcement. He is a good messenger because he comes from a place where people do no have reasons to believe he would be benefiting from such an announcement. The comparison in the role of the messengers between these two pandemics shed light on the importance of choosing the right messenger who most resonate with the people. As we can see during the COVID19 pandemic, the US might not have chosen the best messengers, which contributed to the mistrust that brew nationwide.
Phrases of hope – “I hope that this pandemic ends soon,” or “I hope there will be a vaccine soon,” or “I hope I can find a job again after lock-down ends” or “I hope my family doesn’t catch COVID.”
In the summer of 2020, I myself had religiously uttered these phrases of hope – and every time, it seems to have been answered only with anxiety and worries.
Lessening the worries by trying to stay updated on the latest news didn’t help either – all I got were the words spewed by political leaders downplaying the virus.
“The virus will disappear. It will disappear” (Donald Trump July 21, 2020), while the nation saw an average of 65,000 daily cases.
Many others in positions of power echoed his words.
I remember being paralyzed with fear – an emotional response not unique to just me. Fear erupted all over the US, and continuously up to present day. It puppeted people to lash out at the asian community to “go back where you belong,” or “take the virus back to your commie land.” Fear puppeted people to point fingers at non-vaxxers and non mask wearers – actions that breaks down unity amidst a crisis in which unity is needed the most.
Dr. Sandra Thurmann herself stated that “It’s important to give people hope in the middle of despair.”
There was indeed hope, not from the words of leaders but from actions taking place:
Hope surfaced when the global scientific research community pooled together efforts to produce data for an effective vaccine.
Hope surfaced when new initiatives organized volunteers to safely escort elderly asians leaving their house.
Now, I didn’t expect political leaders to pull a vaccine out of their pocket nor do groundwork with helping in the community; I do expect, however, for them to have the responsibility of communicating some sort of “hope”-esque message to the public, since they know the most of the nation’s current state and its available resources. This leads to the question of the ways a political leader can communicate hope, if they were in such a position where there is indeed hope.
It’s not always apparent that hope does exist in any given moment, since there can be so many unknowns in the pandemic, especially at the start; if hope does not exist, then what is the next best thing to communicate?
Data?
Thoughts and prayers?
Mix of both?
Something else? I personally think that honesty and transparency is the best way to go – but it is easier said than done.
On October 4th, a professor and author named Dr. Steven Thrasher visited our class on his new book tour, The Viral Underclass. His work focuses on different health crises, such as the HIV/AIDS epidemic and the COVID-19 pandemic, to explain how viral underclasses are constructed, Thrasher presents that 12 vectors contribute to this creation: racism, individualized shame, capitalism, the law, austerity, borders, the liberal carceral state, unequal prophylaxis, ableism, speciesism, the myth of white immunity, and collective punishment. Personally, I was quite intrigued about how racism and capitalism (specifically with mass incarceration) play out depending on the health crisis and how they are interlinked. Therefore, I’ve realized that comparing these two vectors will help us understand how history basically repeats itself.
HIV/AIDS
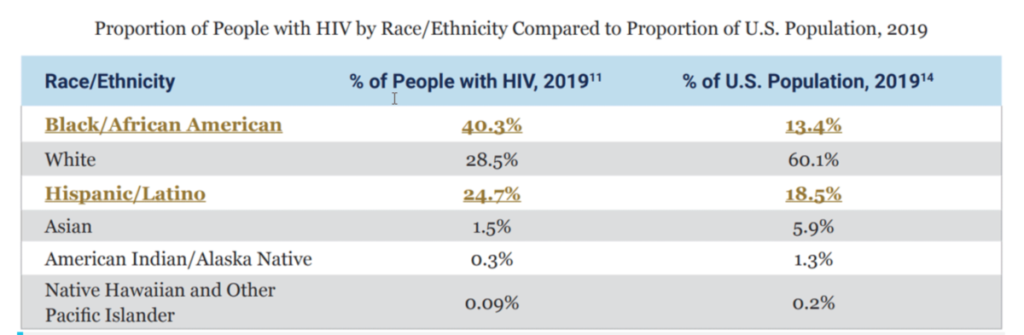
With the HIV/AIDS epidemic, the communities that are the most disproportionately affected are Blacks and Lantix/Hispanics. In these communities, adequate treatment, prevention, and education are not reaching these groups, even though they are the most impacted. Racial discrimination, stigmas, and class status, all influenced by history, are a few factors that have allowed this disproportion to occur. The table below compares the percentage of people within racial groups that have HIV compared to the total population percentage within the US.
Figure 1 Source: CDC
Black/African Americans and Hispanic Latinx people are the two racial categories whose total population percentage with HIV exceeds their total population percentage within the US; this emphasizes how these groups disproportionately experience inequity and inequality due to race during this epidemic.
Another factor that promotes inequity with HIV/AIDS is the capitalistic system that established mass incarceration. Mass incarceration is essentially modern slavery; when the Crack Epidemic occurred in the 80s, most low-income, poor Black communities fell victim to the epidemic and struggled with drug addictions. When the US implemented the “War on Drugs,” the US government heavily targeted Black communities and created laws that targeted these communities and created inequities. One great example of this is the crack vs. powder cocaine disparity which has a 100:1 quantity ratio. Since prisons are private entities, they have practically become businesses that need more prison beds filled to receive more money. Prisons are free labor without any rights, and essentially, the way the system is set up makes them ‘socially dead’ (i.e., unable to partake in society, such as voting, getting jobs, etc.). The author Ruth Wilson Gilmore pinned the term “Golden Gulag” in her book Golden Gulag: Prisons, Surplus, Crisis, and Opposition in Globalizing California to describe the current mass incarceration epidemic within California and further explain how mass incarceration is modern slavery.
According to HIV.gov, they state that “The rate of HIV among prisoners is 5 to 7 times that of the general population. HIV rates are highest among black prisoners. The correctional setting is often the first place incarcerated men and women are diagnosed with HIV and provided treatment.” They also explain that although these incarcerated Black and Hispanic/Latinx communities are at high risk for contracting HIV, most prison facilities haven’t implemented prevention, testing, and treatment options for inmates (HIV.gov). When inmates contract HIV, they might be isolated and prohibited from participating in prison-sponsored activities. Sometimes, their HIV status is not also private and is disclosed to others, promoting discrimination and stigmas to those affected.
With the COVID-19 pandemic, similar experiences and practices within the HIV/AIDS epidemic are seen occurring with this pandemic. In terms of prisoners and those trapped within mass incarceration, they were ignored. Prisoners during the COVID-19 pandemic accounted for extensive infection rates and outbreaks within the country compared to those not incarcerated; yet, those incarcerated had the fewest vaccination rates. In a journal posted by The Lancet, they explain that “According to the COVID Prison Project, state prisons have over three times the rate of COVID-19 infections than the general population, and most of the largest COVID-19 outbreaks in a single site in the USA have been in prisons and jails.’ As discussed with the HIV/Aids epidemic, many of those that are incarcerated are Black/African Americans. Outside of prisons, though, the Black community was still disproportionately affected by COVID-19 more than any other group.
COVID-19
In Black communities, mortality and complication rates within the COVID-19 pandemic have skyrocketed—lack of access to vaccination sites, misinformation and lack of education, and lack of resources/health care are all various components that are influenced by racial division and racism (historically and currently). Data collected from Maritza Vasquez Reyes in their research, “The Disproportional Impact of COVID-19 on African Americans,” explains that “Approximately 97.9 out of every 100,000 African Americans have died from COVID-19, a mortality rate that is a third higher than that for Latinos (64.7 per 100,000), and more than double than that for whites (46.6 per 100,000) and Asians (40.4 per 100,000). Just like HIV/AIDS, the group that needs support and aid the most is the group that receives the least. More data provided by the CDC in Figure 2 help illustrate how disproportionately COVID-19 impacts Black/African-Americans.
Figure 2 “The proportion of deaths from coronavirus 2019 (COVID-19) in African Americans versus proportion of African Americans in state population, from states reporting preliminary data. COVID-19 data are from the COVID Tracking Project [16], and state population demographic data from the US Census.” Website: Pubmed.gov
Opinion
I personally believe that Dr. Thrasher’s 12 vectors are all interconnected, with some even co-dependent. Whether it’s COVID-19, HIV/AIDS, or any other health crisis, without fail, inequities are brought to light and remind us that there is so much more work needed to be done than simply just finding a solution to the health problem. Inequities are a pandemic themselves. Focusing on the United States alone, our history of slavery, discrimination, xenophobia, sexism, and homophobia still plays out today and affects the lives of millions. Whether it’s through a pandemic or hate crimes, these inequities will never be resolved without proper recognition and active improvement on a local, state, and federal level. We need proper funding for these affected communities, educational resources, and basic access to health care. The current legal system, the law of the land, affects everyone single person but yet promotes so much inequality and inequity. We all should understand that to receive equality and justice for all, equity is necessary and makes such a difference.
I was captivated by Steven Thrasher’s emphasis on the words of his colleague, anthropologist Adia Benton: “viruses live briefly in spaces where bodies interface, making the war against the virus is also a war against moments and spaces of connections.” This sentence perfectly paints an explanation for the many social rifts that appeared during this COVID19 pandemic – the “vaxxers vs antivaxxers” or “asians vs Americans” or “maskers vs non-maskers,” and so forth. Likewise during the HIV/AIDs pandemic, it was “straight men vs gay men.” How might a society maintain unity to combat a pandemic while fragmented enough to not facilitate the spread of the virus? Maybe one way is through communication on the boundaries necessary. The CDC during this COIVD19 pandemic, unfortunately, displayed a horrendous communication efforts on the necessary boundaries with their mix-message on masking. It is difficult to fault entirely the CDC for this issue, however, since achieving this balance between unity and fragmentation is no easy task – especially on a nationwide scale. Perhaps as a nation we need to have deep, critical reflections on both the HIV/AIDs and COVID19 pandemic before hints of any resemblance of an answer might appear. With that said, there are good examples of a closer-to-ideal communications that achieves such balance, evident by speech given by the primer minister of New Zealand. Her communication outlined the boundaries in many aspects while also maintaining the message of compassion and kindness to ensure that society remains united against the pandemic rather than pointing fingers internally and creating divisions.
Stephen Thrasher gave an excellent lecture last week on all of the vectors that interact to create the Viral Underclass. Essentially, these 12 components are all pieces to the puzzle of unequal transmission – those most marginalized are most at risk. The Viral Underclass has always existed, but was especially illuminated in these past two years by government response and rhetoric surrounding the COVID-19 pandemic, and something I especially noticed was how COVID-19 is discussed as it relates to ableism.
Source: Disability News Service
Thrasher writes, “In other words, viruses interact with power structures already at play in our society so that those who are already marginalized are left even more susceptible to danger, exacerbating existing social divides.” He goes to write a chapter on ableism astutely titled “Disability as Disposability.” We have seen the ways in which the world has been created to empower the lives and success of able-bodied people. Being left out of the discussion is a common facet of marginalizing groups, and this has been demonstrated time and time again when discussion surrounding COVID-19 response and perception has left out those most impacted by it’s spread.
Source: Catapult
A common line that I heard throughout the pandemic was something along the lines of, “Well, it’s only killing people with comorbidities,” as if those lives are somehow of less value and importance. We can balk at the COVID protocols because it doesn’t impact us, accept that COVID is only hurting those groups. I think there is an implied dismissal of life, specifically for people who are immunocompromised or disabled, sending the message that their lives are not worth following protocols for.
Source: Center for American Progress
I think there is something deeper here, and it’s what Thrasher describes in his book. The common rhetoric of COVID-19 and it’s impact on people with disabilities was accepting, expected, and seemed to be of little concern on the national level. But people with disabilities are 3 times more at risk for death for COVID-19, and that’s not including common intersections like living in poverty or experiencing unemployment. I don’t think people with disabilities faced higher death rates simply because they may have been immunocompromised or had comorbidities; I think unequal and poor quality health access, a societal unwillingness to follow protocols to prevent transmission, and a rhetoric that dismisses the loss of life from your community in the first place put people living with disabilities at such a high risk. To ignore or accept how the pandemic has specifically targeted people with disabilities is to deny them of their humanity, and ultimately, it creates a negative feedback loop of continued marginalization, ostracism, and worse health outcomes.
Last week Dr. Thrasher came into class and discussed his new book, “The Viral Underclass.” I thought Dr. Thrasher raised many interesting perspectives that I had not previously considered. For example, though I learned about the Atlantic Slave Trade during my previous schooling, I never thought of it from a public health perspective. The Atlantic Slave Trade did contribute heavily to the spread of diseases in an unprecedented way, all in the name of profit.
There were other points, like speciesism, which I had never heard of before. I can’t say I fully agree with his logic. In my eyes, human beings are and will always be superior to all other lifeforms on this Earth and deserve priority over those other living beings. However, his point was valid to the extent that we can redefine our relationship with animals to make the world safer and healthier.
Public health scholars have acknowledged several reasons why disease does not impact all groups equally, both globally and within the U.S. Dr. Steven Thrasher takes a deeper dive to research these reasons in his book, The Viral Underclass, where he lists twelve “vectors” that create disparities in cases during viral outbreaks. One reason that particularly stood out to me was unequal prophylaxis. Lack of access to treatment was highlighted on a national and international level during the COVID-19 pandemic. For example, those with lower-income jobs within the U.S. are less likely to obtain health insurance, which would fund COVID-related care. Internationally, higher-income countries were the earliest purchasers of COVID vaccines and were therefore able to vaccinate more people sooner. A lack of access to treatment has been linked to higher rates of infection and death. Therefore, those without the means to obtain prophylaxis are more exposed to COVID, although this same reality could apply to any disease.
Dr. Thrasher highlights unequal prophylaxis as a strong contributor to the viral underclass, but local governments, countries and even international organizations have taken steps toward resolving this inequity. For example, vaccine initiatives such as COVAX, along with the World Health Organization, have helped distributed hundreds of millions of COVID vaccinations to lower-income countries. Earlier this year, many countries have worked, though the World Trade Organization, to grant a TRIPS waiver, which suspends international IP rights of pharmaceutical producers in order to improve vaccine production in lower-income countries. Furthermore, some individuals have traveled to different cities, states, and countries to help provide better testing and treatment access to communities that need it most. Although Dr. Thrasher correctly notes that unequal prophylaxis creates disparities in disease treatment, methods to help the viral underclass have been effective and growing across the world.
Last Tuesday we had the pleasure of listening to Dr. Thrasher speak about the “Viral Underclass”, a concept that had gained traction as the COVID-19 pandemic spread. In the introductory chapter of his book, he quotes his friend: ‘look at the map of COVID-19 rates. It is a map of poverty, racism, and overpolicing. People are dying in jail and because they have been to jail’. This struck me as a critical component of this ‘underclass’.
Last January, I had to opportunity to work inside of Fulton County’s jail to test individuals inside for COVID. We worked in teams to go from unit to unit, to each cell to offer tests. I had never before been so up close and personal to both COVID and the jail system. However, through discussions with these men, so many challenges to maintaining health became apparent. There of course was no where to social distance, no masks available, no regularly administered tests. Many of these men were awaiting trial or sentencing, existing in a limbo and vulnerable to infection.
The pandemic experiences of these men from those on the outside are so starkly different. Incarcerated individuals are infected with COVID at a rate more than five times higher than the nation’s overall rate (Equal Justice Initiative). Then, of course, there’s other factors. Race, poverty, systemic barriers all contribute to the perpetual problem of incarceration. To also allow people to suffer with infection and possibly death while under the supervision of the state is an injustice unlike any other. We know incarceration creates a cycle of oppression, but we have now opened the door to even more lifelong challenges. When the risk of death and long-COVID are added to the equation, there is no aspect of life that is untouched by this inequality.
In our recent class, Dr. Thrasher delivered such an important message surrounding the factors that contribute to and perpetuate the viral underclass. Based on the conversation, I’ve concluded that the vector that is especially influencial is racism. Although there are several other vectors that make up the viral underclass—such as the myth of white immunity and boarders—racism is an underlying cause of many of the other vectors. The strong influence of racism can be seen when we consider that a great proportion of monekypox viral disease cases are among Black/African American people, yet a majority of the vaccines for this disease are going to white people (a phenomenon Dr. Thrasher called the inverse risk prophylaxis). The way that minorities disproportionately make up a high population of incarcerated persons is heavily due to racism—I urge you to check out The New Jim Crow: Mass Incarceration in the Age of Colorblindness, a book that eloquently and thoroughly explains this—which directly contributes to the transmission of disease vector. It’s clear that racism permeates several vectors of the viral underclass. Until we eradicate racism, minority groups will continue to be burdened with health inequities.
Below is an article that further discusses the role of racism in health inequities. I found it to be an interesting, informative read. Hopefully, you’ll find it insightful as well.