To respond to the posts about the HeLa case, I was researching Henrietta Lacks and discovered that coincidentally, a film, The Immortal Life of Henrietta Lacks, will be released on April 22, 2017. It is based Rebecca Skloot’s nonfiction book, The Immortal Life of Henrietta Lacks, a great read. The trailer is below.
“In 1951, cancerous cells from Henrietta Lacks lead to breakthroughs that change the face of medicine forever. Aided by writer Rebecca Skloot, Deborah Lacks embarks on a quest to learn about the mother she never knew.”
“Science took her cells. Her family reclaimed her story. Oprah Winfrey and Rose Byrne star in this adaptation of the critically-acclaimed book. HBO Films presents The Immortal Life of Henrietta Lacks Saturday, April 22 at 8pm on HBO. ”
I look forward to seeing this and wonder how the film is going to respond to the ethics regarding the Lacks case.
Case 8.2: “Ethics and Humanitarian Aid: Vertical Aid Programs”
Introduction
Humanitarian aid highlights tensions in the utilitarian perspective between long- and short-term consequences of actions and policies, and many humanitarian aid workers find themselves acutely torn between deontological and utilitarian ethical perspectives. In this case, Dr. Asadour is a physician attached to a non-governmental organization whose mandate is to participate in a global vertical aid anti-cholera program. Cholera has broken out in a town in South Sudan and the NGO has set up a temporary work station with a Memorandum of Understanding to treat cholera only. Patients with other conditions must be sent to the local hospital, though it is already beyond capacity (Thomas, Waluchow, and Gedge 267).
The Question
As patients line up at the admissions tent, Dr. Asadour must decide whether or not to admit them. Some patients have symptoms that might or might not be cholera, but this cannot be determined unless they are admitted; once admitted, if they do not have cholera, they could nevertheless be treated easily without transfer to the local hospital. The NGO has emergency medical supplies that could save lives of those with non-cholera conditions, such as meningitis. Is it ethical to violate the mandate and treat?
Application:
Challenges Emerging From Resource Scarcity and the Need to Allocate Them
I came across “Ethics in Humanitarian Aid Work: Learning from the Narratives of Humanitarian Health Workers,” a qualitative study drawing on Grounded Theory analysis of 20 interviews with health care professionals who have provided humanitarian assistance; I found the predicaments that it presents to be applicable to this case.
The study reveals that respondents persistently were confronted by situations in which the resources available were insufficient or inadequate—insufficient to sustain life, or inadequate in relation to people’s needs. The choices that scarce resources presented were a recurring source of ethical struggle. Describing her work at an urban hospital in the Caribbean, R19 (RN) said:
“Whenever you see so many sick [people] and you realize that there are some that have to be turned away then you do say okay well we need to triage and we need to decide you know who we’re going to treat” (Schwarz et. al.).
She raised questions about the rightness of vertical aid, yet explained that over time she came to believe that refusing care to some was justified to ensure care for others. In many instances, professionals chose to offer resources to the people perceived to have the best chance of survival (Schwarz et. al.).
Challenges of resource allocation were most acute when patients’ lives were at stake. But care resources for chronic conditions were also scarce. Here, too, respondents faced situations in which they had to choose who would receive care. The deciding itself was often morally difficult, as were the consequences of the decisions. R10 (physical therapist), for instance, brought funds from friends at home to support the health needs of the people in Central America with whom she worked. In one way, she said, money gave her options for problem solving—she might purchase the services of a local person to create a chair that allowed a child with a disability to sit upright, for instance. But in another way, “It created more problems because people had given me all this money in the faith I would do the right thing with it and I didn’t know exactly what the right thing was” (Schwarz et. al.).
Challenges Emerging From Aid Agency Policies and Agendas
Treating people’s chronic conditions is outside the remit of some agencies. In vertical programs, treatment is only provided to individuals who have specified health conditions that match pre-established priorities. Even where adhering to the agency policy was judged on balance to be the ethically correct act, it could still be difficult to do (Schwarz, et. al.).
What about Beneficence?
As we have discussed in class, beneficence demands that we actively promote the well-being of others and prevent or remove harm to them (Vaughn 10). Accordingly, there is little doubt that the health care professionals have such a duty to advance patients’ welfare, promote their well-being, and prevent or remove harm to them. To what extent does the principle of beneficence justify violation of the mandate?
In the Media
TEDxHamburg – Linda Polmann – “What’s Wrong With Humanitarian Aid? A Journalist’s Journey”
This is a general discussion provided by TEDx on the ethical dilemmas associated with humanitarian aid. What, then, is the solution?
Conclusion
Sometimes, refusing care to some is justified to ensure care for others.
In some instances the policy, or following it, is felt to be too significant a violation of other ethical obligations.
The desire to help a particular patient—a woman with diabetes, for example—outweighs an agency directive against providing treatment deemed unsustainable in the context, a situation that tests perceived duties of beneficence against policies on scarce resource allocation.
Works Cited
Schwarz, Lisa, et. al. “Ethics in Humanitarian Aid Work: Learning From the Narratives of Humanitarian Health Workers.” AJOB Empirical Bioethics, 2010, 1(3): 45-54. Web. 9 April 2017.
Thomas, John E., Wilfrid J. Waluchow, and Elisabeth Gedge. “Case 8.2: “Ethics and Humanitarian Aid: Vertical Aid Programs.” Well and good: a case study approach to health care ethics. Peterborough, Ontario: Broadview Press, 2014. Print.
Vaughn, Lewis. Bioethics: Principles, Issues, and Cases. New York: Oxford University Press, 2010. Print.
Case 7.4: “Access to Experimental Drugs in Catastrophic Circumstances”
Introduction
The role of the government in regulating access to drugs and the ethical norms governing clinical trials have been challenged and debated in bioethics and legal circles. Certain assumptions about the ethics of running clinical trials were brought under scrutiny especially during the late 1980s when AIDS was assuming epidemic proportions and pressure was building to find effective therapies.
In this case, Harold has AIDS and is rejected as a candidate for a clinical trial of an antiretroviral drug because his health status is poor. “[He] had everything to lose by accepting the rules and nothing to lose by trying to get around them” (Thomas, Waluchow, and Gedge 256). Harold forms a group of advocates that offers an open arm alternative to the double-blind clinical effect; participants consent to receiving the drug and are monitored for outcomes.
The Question / Discussion
Having an open arm offers patients an opportunity to exercise a high degree of autonomy in assuming a significant risk; it also enhances the autonomy of those entering the clinical trial as well, since they now have the option of either arm as a way of accessing the experimental therapy. Does the principle of autonomy mean that very ill people should be able to access any drug they wish if they accept the risk?
Autonomy
In Bioethics: Principles, Issues, and Cases, Vaughn argues that the heart of the modern doctrine of informed consent in Kantian. I agree with Vaughn that because persons are autonomous, rational agents, they must be allowed the freedom to make choices and to have them respected; they may give or withhold their consent to medical treatment and the risks of research—consent that is valid only if informed, competent, and voluntary (Vaughn252). Autonomous agents have the right to decide for themselves whether to expose their persons to the rigors and risks of clinical investigations.
Ethical Justification of Having an Open Arm
Access to the open arm, an ethical alternative to doing nothing for those like Harold who are catastrophically ill, has an ethical justification; although it is not designed to produce the kind of generalizable knowledge that issues from a clinical trial, it will provide clinical information on a case by case basis, which may in time reveal useful commonalities or surprising individual results worth developing into a further research question. Further, it is often considered compassionate, since it offers the possibility of a cure to those in very dire circumstances (Thomas, Waluchow, and Gedge 257).
Application:The Tuskegee Tragedy
https://www.youtube.com/watch?v=-JP3Qa32IPw
The shocking revelations about the Tuskegee Study came decades after the research had been conducted. When finally told, the story provoked outrage, moral debate, and an apology from President Bill Clinton (Vaughn 241).
The Public Health Service, working with the Tuskegee Institute, began a syphilis study in 1932. Nearly 400 poor black men with syphilis from Macon County, Ala., were enrolled in the study. They were never told they had syphilis, nor were they ever treated for it. According to the CDC, the men were told they were being treated for “bad blood,” a local term used to describe several illnesses, including syphilis, anemia, and fatigue (Vaughn 241).
At the start of the study, there was no proven treatment for syphilis. But even after penicillin became a standard cure for the disease in 1947, the medicine was withheld from the men. The Tuskegee scientists wanted to continue to study how the disease spreads and kills. Dozens of the men had died and many wives and children had been infected. It wasn’t until 1997 that the government formally apologized for the unethical study: “What was done cannot be undone. But we can end the silence. We can stop turning our heads away. We can look at you in the eye and finally say, on behalf of the American people: what the United States government did was shameful” (Vaughn 241).
Connection and Conclusion
Unlike in Case 7.4, moral principles were not upheld during the experiment conducted in this historical case. Autonomy (respect for persons as autonomous agents) beneficence (doing good for and avoiding harm to persons) and justice (treating equals equally) were violated. By inference, a very ill patient like Harold should be able to access an experimental drug as an autonomous person if he accepts the risks; he must be competent and consent must be both voluntary and informed, while autonomy, beneficence, and justice have to be weighed out and upheld.
Works Cited
Beauchamp, Tom L., and James F. Childress. Principles of Biomedical Ethics. New York: Oxford University Press, 2013. Print.
Thomas, John E., Wilfrid J. Waluchow, and Elisabeth Gedge. “Case 7.4: Access to Experimental Drugs in Catastrophic Circumstances.” Well and good: a case study approach to health care ethics. Peterborough, Ontario: Broadview Press, 2014. Print.
Vaughn, Lewis. Bioethics: Principles, Issues, and Cases. New York: Oxford University Press, 2010. Print.
Physician-assisted suicide is one of various types of end-of-life decisions debated in bioethics and legal circles. In this case, Sue Rodriguez has ALS. Once she began to experience deterioration of her abilities, she entertained the possibility of suicide and petitioned the courts for an order “which would allow a medical practitioner to set up technological means by which she might […] end her life.” After the Supreme Court of Canada issued its ruling, she took her own life with the assistance of an unidentified physician. In 2012, Gloria Taylor suffered from the same disease that affected Sue and brought the issue to the forefront of the Canadian public once again (Thomas, Waluchow, & Gedge 214).
The Question / Discussion
Like many of those we have discussed in class, this case presents a question about the morality of the choice of a physician to assist suicide, not directly about the legal issue; setting aside the legal question, which regards social policies and actions of the political community as a whole, if you or I were a physician, would it ever be morally right for us to choose to assist someone to commit suicide? (Lee 213).
Life and death: a choice
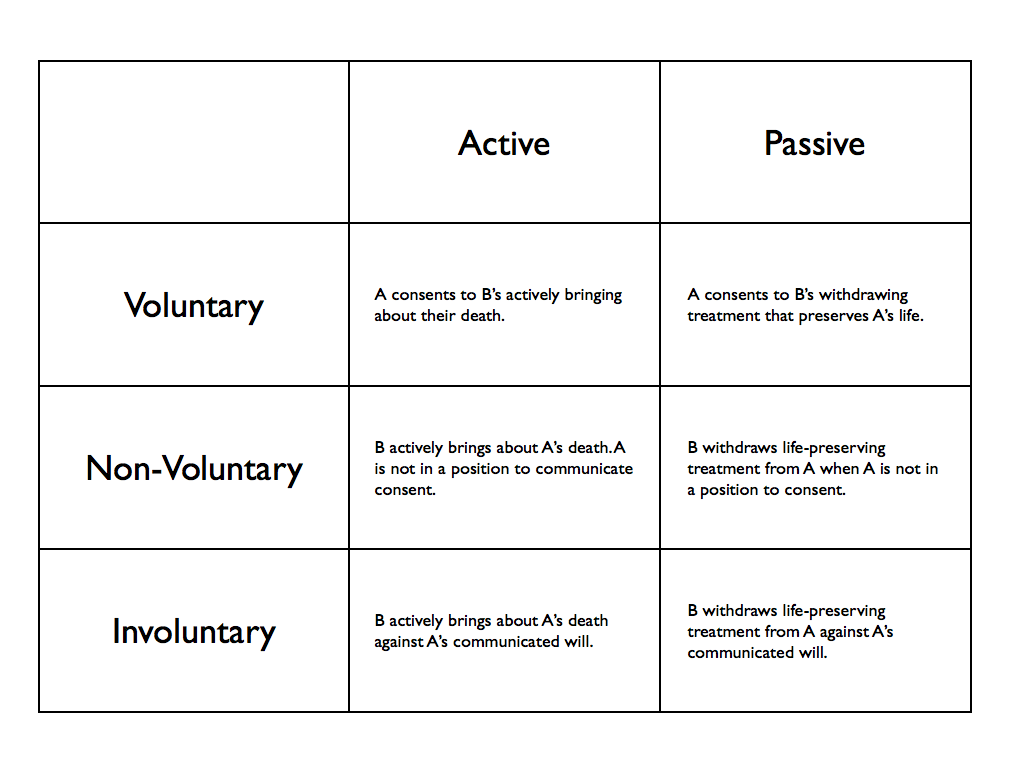
Intentional Killing vs. Accepting Death as a Side Effect
Active and Passive Measures
Contemporary Debates in Bioethics presents two perspectives: “Physician-Assisted Suicide is Ethical,” and “Physician-Assisted Suicide is Not Ethical.” It is important to understand that we do not always have to take all measures possible to preserve someone’s life, our own included. It can be morally right to forgo life-sustaining treatment, foreseeing that this will result in dying more quickly than one otherwise would. There is a crucial distinction between intentionally killing and choosing to forgo treatment, foreseeing (but not intending) the death or hastening of death, that will occur as a side effect. Sometimes not doing something can be chosen as a means of bringing about some end. So, it is possible to choose an omission as a way of bringing about someone’s death. In choosing to assist Sue with suicide, the physician diminished his respect for the intrinsic good of human life (Lee 215).
Hence, I agree with Patrick Lee in arguing that physician-assisted suicide is not ethical. It would have been acceptable for the physician to withhold treatment and allow Sue to die (passive euthanasia), but that it was not acceptable for him to assist her in committing suicide (active euthanasia).
In the Media Today / Discussion
This case brought to mind two films that many may have seen: You’re Not You and Me Before You.
You’re Not You is a drama centered on a classical pianist named Kate who, like Sue, has been diagnosed with ALS. When Kate is in the advanced stages of ALS, she is shown sitting upright in her wheelchair and speaking in a labored fashion. The film is valuable in showing the way in which patients in this condition are unable to sit upright because the muscles in their backs are no longer receiving signals from the brain; the same is true of the muscles in the throat and jaw, making speech impossible. Kate says, “I’m going to die. I don’t want to be here.” Do you think that if misery is placing an undue burden on her existence, she may ask for assistance in ending her life? Trailer:
In Me Before You, the lead character is disabled (paralyzed) and chooses to end his life, leaving the newfound love of his life instructions to “live boldly” and encouraging her to live well. I feel that this romanticizes a death wish and promotes suicide as an act of love. What message do you think this sends, and how does his predicament relate to Sue’s case? Should medical aid in dying be considered differently for people with disabilities (Will) than people with terminal illnesses (Sue)? Trailer:
Works Cited
Beauchamp, Tom L., and James F. Childress. Principles of Biomedical Ethics. New York: Oxford UP, 2013. Print.
Lachs, John. “Physician-Assisted Suicide is Ethical.” Contemporary Debates in Bioethics. Chichester, West Sussex: John Wiley & Sons, Inc., 2014. Print.
Lee, Patrick. “Physician-Assisted Suicide is Not Ethical.” Contemporary Debates in Bioethics. Chichester, West Sussex: John Wiley & Sons, Inc., 2014. Print.
Thomas, John E., Wilfrid J. Waluchow, and Elisabeth Gedge. “Case 6.2: Sue Rodriguez: ‘Please Help Me to Die.'” Well and good: a case study approach to health care ethics. Peterborough, Ontario: Broadview Press, 2014. Print.
Withholding Information: An Introduction to the Moral Issue
Issues of truthfulness and disclosure are among the most difficult and delicate ethical issues for healthcare professionals. Nurses in trauma centers face distinct ethical challenges as questions arise about whether withholding information to patients is ever justified. After reading Tom L. Beauchamp’s “There Are Circumstances in Which a Doctor May Withhold Information” from Arp and Caplan’s Contemporary Debates in Bioethics, I will present the paternalistic and therapeutic privilege approaches to this case to suggest that trauma nurses and other healthcare professionals have an obligation to manage information in a way that “sometimes withholds information and at other times stages disclosures over time” (Arp and Caplan 409).
The Case
“Case 3: Emergency and Trauma Nurses: When to Give Bad News” explores the question of when to tell the truth in situations when, given the patient’s physical and psychological condition, delivering devastating news might potentially jeopardize a patient’s health, and possibly life. In this case, Amira is driving on the highway with her partner, Casey, and their daughter, Samantha; they are hit by a drunk driver in a multi-vehicle accident. Casey’s vital signs are absent, while Amira, unaware of her partner’s death, is in the trauma room in need of surgery. When she asks about Casey, the nurses fear that stress may further impair her capacity to survive the surgery; they are also afraid that she may die in the operating room without knowing the truth about her partner (Yeo, Moorhouse, and Khan).
The Best Response:
A. Paternalistic Approach
Paternalism is the intentional overriding or limitation of one person’s autonomous choices or actions by another person or institution, where the latter justifies the action-a nurse’s withholding information-by appeal to the goal of providing a benefit or of preventing or mitigating harm to the person whose choices or actions are limited or overridden (Arp and Caplan 413). The motivation is therefore “the beneficent promotion of physical or psychological health and welfare of those whose autonomous choice is limited or overridden” (Arp and Caplan 414). The moral thesis is that as risk to Amira’s welfare increases, the likelihood that withholding information is justified correspondingly increases.
B. Caring for Patients Who Have Received Bad News: Therapeutic Privilege
The primary concern of emergency and trauma nurses should not at the onset be the disclosure of all available pertinent information. While some information can be delayed, some of it may justifiably never be mentioned (Arp and Caplan 415). The trauma nurse’s fundamental obligation at the beginning of the process of disclosure is to calm down and reassure Amira, while engaging sympathetically with her feelings and conveying the presence of a caring, knowledgeable medical authority (cf. Quill and Townsend, 1991). The nurse’s emotional investment in the feelings of the Amira should be joined with a detached evaluation of what the patient’s medical and informational needs are; cases in which the risk of harm and burden will be substantially increased if all pertinent information is disclosed call for a “skilled management of each item of information” (Arp and Caplan 415). Moreover, how should the trauma nurses decide how and when Amira should be told the bad news about her partner?
Based on the therapeutic privilege, there is a commonly understood and “morally intuitive difference” between lying to someone with the intention to deceive and withholding the truth from someone to “avoid a perceived negative, detrimental, or painful physical or psychological consequence” (Arp and Caplan 404). Considering Amira’s best interest, can disclosure of Casey’s death therefore be delayed justifiably?
Contemporary Issues: Skilled Management of the Truth — Not Always Justifiable
Harvard University’s Justice with Michael Sandel presents “A Lesson in Lying.” Sandel discusses the realm of freedom and the realm of necessity as well as the carefully worded denials in the Monica Lewinsky affair of Bill Clinton (~16 minutes). Although skilled management of the truth is not always justifiable, in the case of Amira, the decision of a trauma nurse to withhold information is founded on the best interest of the patient. As Sendel discusses, in the light of Kant, is there something morally at stake in the distinction between a lie and a misleading, but true evasion? If so, is this adequate for rendering information withholding by healthcare professionals morally impermissible?
Works Cited
Arp, Robert, and Arthur L. Caplan. Contemporary Debates in Bioethics. Chichester, West Sussex: Wiley Blackwell, 2014. Print.
Quill, T, and Townsend, P. (1991). Bad news: Delivery, dialogue, and dilemmas. Archives of Internal Medicine, 151, 463-464.
Yeo, M., A. Moorhouse and P. Khan. “Case 3: Emergency and Trauma Nurses: When to Give Bad News.” Concepts and Cases in Nursing Ethics.