“Atnafasy! Atnafasay…. Yalla, Adfa3ee!” These Arabic phrases echoed in the delivery room, creating an intriguing rhythmic tone that aligned with the beeps coming from the hospital machines. In a room bustling with healthcare professionals, only the grandmother and I engaged in this back-and-forth dialogue, encouraging the mother-to-be on the hospital bed to continue pushing.
As the machines beeped and tension filled the air, I found myself reciting what felt like a chant or pep talk. The grandmother, sensing the gravity of the situation, raised her hands in prayer. In the midst of this, a soon-to-be mother prepared for childbirth, and I, unexpectedly, became the conduit between medical jargon and family understanding.
How did I end up here?
Volunteering as a labor support volunteer often means signing up for more than you expect. The 5-hour training at Emory nursing school covered the basics – stages of birth, different pregnancy phases, cultural sensitivity, and even educational videos of live births. I walked in anticipating a medically focused experience, similar to nursing or midwifery—but to my surprise, the role unfolded into much more than just that. As a labor support volunteer, you were to be paired with a pregnant refugee mother. Your responsibilities involved not only accompanying her to prenatal appointments but also offering translation whenever possible and advocating for her medical preferences. More importantly, the labor support volunteer would have to advocate for the mother in the hospital during the labor.
But with my partner, it went beyond just transportation and translation—we chatted during the car drives to her appointments, watched TikToks together in waiting rooms, and shared coffee at her home after appointments. The title “Labor Support Volunteer” hardly does the experience justice.
Speaking Arabic added an extra layer to the experience, fostering a deeper connection with mothers like Lana from Syria. Going to Lana’s house felt like stepping into a second home, surrounded by Moroccan couches, Persian rugs, and vibrant red curtains.
Layout of coffee, apricot juice, prenatal vitamins, biscuits, surrounded by persian carpeting and moroccan couches.
I became acquainted with her family, sharing in all their delights – from Arabic coffee to basboosa, a traditional Arab dessert I’d always craved. It was as if I had become a close family friend, always ensured to be well-fed—they would never allow me to leave without a finished plate!
The ambiance was completed by their five outdoor kittens, greeting me with the kindest eyes.
As I fed the cats leftover food, I would speak in Arabic with Lana, her mother-in-law, and her sisters about memories of Syria and the yearning for home, interspersed with discussions about Lana’s pregnancy. This unique experience, unlike any other, allowed me to work with patients longitudinally, proving to be invaluable on the day of Lana’s birth.
One early morning, after taking Lana to her prenatal appointment, I had expected to return her home and quickly drive to campus ready for my first lecture of the day. Fate had other plans: we received unexpected news from the doctor – she was in labor! Aware of her birth plan, I immediately drove her from the clinic to the downtown hospital, doing my best to maintain composure. When questioned about why I was accompanying her, Lana interrupted, stating that I was her friend. More than a labor support volunteer, more than an interpreter, I had become a friend to Lana.
The 12-hour procedure unfolded with communication with nurses and doctors, along with shared jokes with Lana’s mother and her husband. Throughout this challenging journey, particularly for Lana as a first-time mother, I improvised translations for terms like “contractions” and “push.” Finally, at around 10:00 PM, a baby girl was born, and Lana’s grandmother insisted I stay until I had tried her freshly cooked shawarma sandwiches.
It was more than a job; it felt like home, like being part of my family from the Middle East. These stories opened my eyes to the real experiences of refugee women, shedding light on the challenges they face in accessing healthcare. As I started feeling like a member of their family, it sparked a curiosity in me to dive into the cultural aspects of family and parenthood within refugee identities. This newfound perspective is pushing me to explore more about the human right to fertility for refugees, not just as an academic pursuit but as a way to understand and advocate for the people I’ve come to know and care for.
My personal journey with Lana and her family has inspired a broader quest—to understand, empathize, and amplify the voices of refugee women in their pursuit of motherhood. As I relate back to my research, this experience has illuminated the importance of human connection, family dynamics, and cultural understanding in addressing the barriers that refugee women encounter in their healthcare journeys. Through these narratives, I hope to contribute to a larger conversation on reshaping healthcare systems to be more inclusive, compassionate, and responsive to the diverse medical needs of refugee communities in America.
Students and co-instructors of IDS 290: Narrative Medicine at Emory University for the Fall 2023 semester.
You show up to the doctor’s office because you have a headache, fatigue, joint pain, and the overall feeling that something’s just not right. You tell your doctor all this but keep the last part to yourself because you feel it would make no difference. The doctor asks if you have a fever, cough, sore throat, or have traveled out of the country in the last two weeks.
You answer, “no”.
She asks you if you’re active, and you say, “Yes, I went on a run yesterday actually.”
“Did you drink enough water?”
“I guess it’s possible I didn’t.”
“Drink plenty of water and electrolytes and try to take it easy for the next few days. You may just be dehydrated.”
It doesn’t feel like dehydration, but you nod and agree because she’s the doctor—she’s supposed to know better than you. You leave the office without mentioning the hike you went on in Maine last week because your doctor didn’t ask—she may have tested you for Lyme Disease otherwise.
The incomplete nature of this interaction is not unique, it is the norm. It’s difficult to open up to someone you only see once a year for fifteen minutes, even when they do ask the right questions. It’s even harder to give someone information unprompted, especially when you feel it’s not important. Because of this, your doctor didn’t have the whole story; perhaps she didn’t have the time to find out, or perhaps she didn’t know to ask. They don’t teach doctors to make small talk with their patients in college or medical school, so how could they not be strangers to their patients if they don’t learn how to get to know them?
It’s difficult to come across other social interactions where revealing sensitive health information to a stranger is the expectation and the norm. So how do doctors learn to build trust with their patients within the time constraints of an appointment? It certainly isn’t through their college education.
In the United States, undergraduate premedical students must complete extensive coursework in biology, chemistry, physics, and math. The traditional approach to science education seldom contextualizes information within a broader social and cultural setting, leaving students ill-prepared to understand and interpret patients’ stories. Rita Charon provides a framework for physicians to engage with patients’ social and cultural backgrounds in her narrative medicine model of medical practice to supplement the biomedical knowledge student-doctors acquire in their undergraduate and medical school studies. Dr. Charon’s model uses narrative competence – the ability to acknowledge, absorb, interpret, and act on the stories of others – to connect physicians to patients’ illness experiences.[1] Such engagement with patient narratives opens opportunities for physicians to enhance their knowledge of their patients beyond family history questionnaires and physical exam findings in creating treatment plans. Dr. Charon’s model represents a holistic approach to medicine that the current undergraduate premedical curriculum fails to address.
To help fill this gap in the undergraduate premedical curriculum, I designed a narrative medicine course for undergraduate students pursuing healthcare careers based on Dr. Charon’s narrative medicine model. Class activities included in-class journaling, spoken personal statements, reading discussions, ethical case studies, and conversations with physicians and medical students. The goals of this course were to introduce the concept of narrative medicine, encourage reflection about the role of the physician in the doctor-patient relationship, and engage in learning from others’ experiences, or in other words, their stories. In end-of-course evaluations, one hundred percent of students responded, “strongly agree”, to the statement, “I have learned more from others’ experiences (classmates, visiting physicians, etc.) in this course.” This is a hopeful step in the direction of educating future doctors on how to learn from others’ stories. By offering more classes like this one at colleges and universities across the country, we can strive toward a future in medicine where physicians value learning from each other and their patients as much as the sciences.
[1] Rita Charon, “Narrative Medicine: A Model for Empathy, Reflection, Profession, and Trust,” JAMA 286, no. 15 (October 17, 2001): 1897–1902, https://doi.org/10.1001/jama.286.15.1897.
The history and contention surrounding the commercial sex trade is reflected in its most basic form: its terminology and definitions. These definitions, terminology, and their direct relation to where perceived power reveal just how difficult it is to talk about the issue without confronting the legacy of the feminist sex wars of the 1970s and 1980s.
(Photo credit: Irin Carmon)
The feminist movements of the 1970s and 1980s were marked by passionate debates surrounding sexuality, pornography, and the sex industry, collectively known as the “Feminist Sex Wars.” These ideological clashes among feminists significantly influenced contemporary discussions on prostitution and commercial sex work.
In navigating this legacy, the feminist sex wars are often reduced to a black-and-white debate between “exploitation” versus “empowerment,” (Comella, 459) conceived of as a straightforward conflict between antipornography feminists on one side and pro-sex feminists on another, respectively.
(Photo credit: Kim Samuel)
This polarization, tied directly to media narratives surrounding sexuality (Bracewell, 24), often portrays sex workers as either “helpless victims or empowered escorts with unfettered agency” (Comella, 459). Through this framing, the complexities of sex workers’ lives and experiences are ultimately reduced to something eye-catching, inflammatory, and palatable. So let us explore what are these ideas that still influence policy:
1. Autonomy and Choice:
The most notable spark of contention within the Feminist Sex Wars is the terminology between “sex work” and prostitution.”Anti-pornography feminism argued that pornography and certain sexual practices, including sex work, were forms of violence against women. They believed that these activities perpetuated harmful stereotypes, objectified women, and reinforced patriarchal power structures (Catharine MacKinnon and National Organization for Women). Sex-positivist feminists, on the other hand, including activists like Gayle Rubin, sought to challenge this more conservative and moralistic attitude within feminism. They emphasized sexual agency, autonomy, and the right of individuals to make choices about their own bodies and sexual practices without moralistic judgments, viewing prostitution as sex work and inherently an “occupation” (Rubin, 150). The discourse between these two branches of feminism, antipornography and pro-sex, established many of the core arguments used in contemporary sex trade discourse, and their respective terminology directly relates to where on views power, consent, and agency within the commercial sex trade.
(Photo Credit: Teen Vogue)
2. Legal Frameworks and Decriminalization:
The sex-positive feminist stance has contributed to the push for decriminalizing sex work in various parts of the world. Activists argue that decriminalization would enhance the safety and well-being of sex workers by allowing them access to legal protections and basic labor rights. Conversely, anti-prostitution feminists often contend that decriminalization could perpetuate gender-based violence and exploitation. Anti-pornography feminists Andrea Dworkin and Catherine MacKinnon, in contradiction to decriminalization, argued that the law could be used in the protection of women to work against gender-based violence.
3. Sexuality and Empowerment:
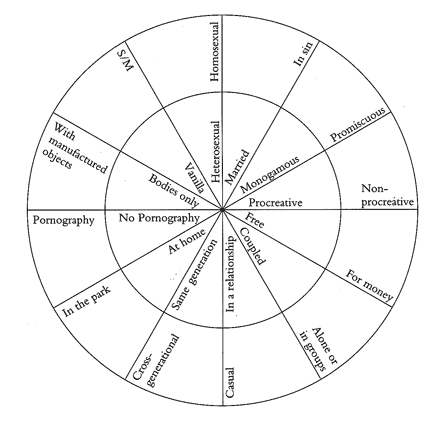
The sex-positive feminist perspective has influenced contemporary discussions by emphasizing the importance of recognizing and respecting diverse forms of sexual expression and labor. This viewpoint challenged the traditional narrative that frames all sex work as inherently degrading and disempowering, promoting the idea that some individuals may find empowerment and economic independence through their work in the sex industry. A key example of this is the charmed circle by Gayle Rubin, that critiques dominant sexual norms and the hierarchy of sexual deviance versus sexual acceptance.
Let us continue with Gayle Rubin’s Charmed Circle…
The charmed circle depicts the hierarchy of dominant, acceptable sexual norm. Heterosexuality, monogamy, and “free” (Rubin, 157) are deemed not only acceptable but the only acceptable sexualities according to dominant sexual norms. Other sexualities that can be perceived as deviant to this, like homosexuality, BDSM, and sex for money (prostitution) are marginalized, stigmatized, and placed on the outskirts of our society, as shown by their placement at the outer layers of the circle. (Photo credit: Rubin, 157).
Rubin’s arguments against the moralistic condemnation of non-normative sexual practices, including sex work, advocate for a more inclusive and tolerant approach that moves beyond previous conservative feminist ideas that sex workers are helpless and without agency.
This outlook was and continues to be questioned: If a woman begins working in prostitution before they are an adult, participate in it due to fear of violence from their pimp or partner (Giobbe 33), or are participating in the trade due to dire financial circumstances (including prostitution being the sole option for financial independence) (Monto, 162), is it a choice?
The Feminist Sex Wars was, in many ways, the beginning of the critical feminist and legal interrogation into where consent and power lies in the commercial sex trade. The Feminist Sex Wars of the 70s and 80s played a pivotal role in shaping the contemporary discourse on prostitution and commercial sex work. The clashes between anti-pornography feminists and sex-positive feminists have left a lasting imprint on the feminist movement, contributing to a more nuanced and complex understanding of the issues surrounding sexuality, agency, and empowerment within the context of the sex industry.
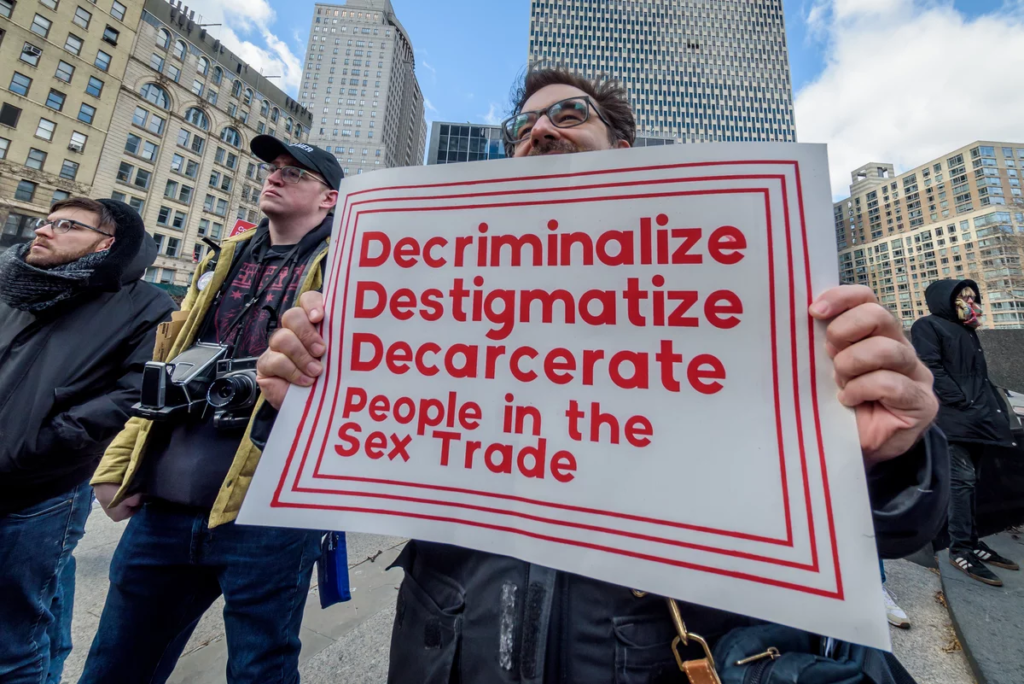
(Photo credit: Garsd)
References
Bracewell, Lorna Norman. “Beyond Barnard: Liberalism, Antipornography Feminism, and the Sex Wars.” Signs: Journal of Women in Culture and Society 42, no. 1 (2016): 23–48.
Carmon, Irin. “Who Actually Lost the Sex Wars?” The Cut, August 12, 2022. https://www.thecut.com/2022/08/the-sex-wars-sexual-culture-today.html.
Comella, Lynn. “Revisiting the Feminist Sex Wars.” Feminist Studies 41, no. 2 (2015): 437–62.
Garsd, Jasmine. “Should Sex Work Be Decriminalized? Some Activists Say It’s Time.” NPR, March 22, 2019, sec. Business. https://www.npr.org/2019/03/22/705354179/should-sex-work-be-decriminalized-some-activists-say-its-time.
Giobbe, Evelina. “An Analysis of Individual, Institutional, and Cultural Pimping.” Mich. J. Gender & L. 1 (1993): 33.
Lancaster, Roger N. Sex Panic and the Punitive State. Univ of California Press, 2011.
MacKinnon, Catharine, and National Organization for Women (NOW). “MacKinnon Q & A NOW’s Views on Decriminalization.” National Organization for Women, 2019. https://now.org/wp-content/uploads/2019/11/Comms-Team-QA-1.pdf.
Monto, Martin. “Female Prostitution, Customers, and Violence.” Violence Against Women 10, no. 2 (2004): 160–88. https://doi.org/10.1177/1077801203260948.
Rubin, Gayle S. “Thinking Sex: Notes for a Radical Theory of the Politics of Sexuality.” In Culture, Society and Sexuality, 143–78. Routledge, 2002.
Samuel, Kim. “The Stigmatization Behind Sex Work.” Samuel Centre For Social Connectedness, May 4, 2018. https://www.socialconnectedness.org/the-stigmatization-behind-sex-work/.
Weeks, Jeffrey. Sexuality and Its Discontents: Meanings, Myths, and Modern Sexualities. Routledge, 2002.
“Why Sex Work Is Real Work | Teen Vogue.” Accessed December 10, 2023. https://www.teenvogue.com/story/why-sex-work-is-real-work.
Imagine you are a college student, sitting in your Biology class, when your Emergency Medical Services (EMS) radio blares. You gather your belongings and hastily leave class — attempting to not cause too much of a distraction. You meet your partner at your truck outside the building to learn that the call is high acuity: a cardiac arrest. With lights flashing and sirens blaring, together you race to the dispatched location. Cardiac monitor, medications, and advanced airway measures in hand, you calmly but diligently proceed to the location – determined to save a life. You are the first ones to arrive on scene. You knock on the door announcing yourself and then enter. Limp on the couch, blue and cold, no pulse and with obvious signs of death you find your classmate. Your bag drops. Your heart sinks. Yet, there is no time to feel. Beside him. you see his parents, screeching, crying, on their knees. You crouch down, hold their hand, and inform them that their child has passed away. “We regret to inform you that your son has passed away. We are so sorry for your loss.”They fall into your arms. You hold them till the police and other agencies arrive. You give a report and fill out paperwork. And then you return to class.
On many campuses across North America, collegiate EMS organizations (CBEMS) provide emergent prehospital care to their communities. The anecdote above is from a call I experienced working as an Advanced Emergency Medical Technician (EMT) for my university’s collegiate EMS organization. Many collegiate student EMT providers can recount difficult experiences of responding to one’s peers, ranging from alcohol intoxication, anaphylaxis, overdoses, traumas, and more. EMTs are typically faced with significant physical and psychological stressors, with frequent exposure to traumatic events, with little to no closure. CBEMS providers must balance an already grueling profession with the demands and rigor of a college education. Current coping mechanisms generally used by prehospital providers largely center around repression of feelings, dark humor, peer communication, and avoidance (Alexander & Klein, 2001). These are not the most beneficial are actually correlated with more psychological problems (Brown et al., 2002). Thus, methods that mitigate traumatic stress symptomatology and serve as proactive measures are needed and essential for both provider and patient safety. Preventative measures for this group are even more necessitated due to their significant potential benefit, given that this population is only at the forefront of their careers.
Mindfulness and contemplative practices have exploded in the past few decades and research has followed. These may be particularly beneficial among these burdened populations. CBCT (Cognitively-Based Compassion Training) presents a experimentally tested framework for mindfulness. CBCT is derived from the Indo-Tibetan Buddhist lojong (Tib: བློ་སྦྱོང་, Wylie: blo sbyong) or mind-training tradition and was adapted to be accessible to those of any or no faith tradition. As is evident in its’ name CBCT is a “cognitive” or “analytical” style of meditation that combines exercises for stabilizing attention with contemplation of aphorisms, visualizations, self-inquiry, and related meditative exercises for cultivating and reinforcing compassion. It has experimentally been shown to decrease depression, loneliness, and stress-induced inflammation while increasing compassion, empathy, and hopefulness(Pace et al. 2012)(Dodds et al. 2015)(Lang et al. 2019)(LoParo et al. 2018)(Reddy et al. 2013).
CBCT was developed by Lobsang Tenzin Negi, Ph.D., a Associate Teaching Professor in the Department of Religion, former monk, and co-founder and executive director of the Center for Contemplative Sciences and Compassion-Based Ethics (CCSCBE) at Emory University. The goal of CBCT is to challenge and examine feelings and actions towards others with the goal of generation spontaneous empathy and compassion for oneself and others (Pace et al. 2012). CCSCBE focuses on educating the heart and mind through innovative research frameworks. The center reflects Emory’s collaborations with His Holiness the Dalai Lama since 1998.
CBCT has been a catalyst for positive change across various groups, spanning veterans, medical students, and hospital chaplains. With this momentum, there is a compelling prospect that it will play a pivotal role in elevating conditions for collegiate EMTs, their patients, and beyond.
“You may want to analytically meditate on how you might have contributed in some way to the situation that made you angry. And while the midst of anger, your tendency is to perceive the person who harmed you as 100% bad. But deeper analysis will make you realize that every human being is composed of both positive and negative characteristics, and you can try to get a more realistic view of the person, thereby diluting the anger harbored against the person.” — Dalai Lama
Alexander, D. A., and S. Klein. 2001. “Ambulance Personnel and Critical Incidents: Impact of Accident and Emergency Work on Mental Health and Emotional Well-Being.” The British Journal of Psychiatry: The Journal of Mental Science 178 (1): 76–81. https://doi.org/10.1192/bjp.178.1.76.
Brown, Jill, Gerry Mulhern, and Stephen Joseph. 2002. “Incident-Related Stressors, Locus of Control, Coping, and Psychological Distress among Firefighters in Northern Ireland.” Journal of Traumatic Stress 15: 161–68. https://doi.org/10.1023/A:1014816309959.
Dodds, Sally E., Thaddeus W. W. Pace, Melanie L. Bell, Mallorie Fiero, Lobsang Tenzin Negi, Charles L. Raison, and Karen L. Weihs. 2015. “Feasibility of Cognitively-Based Compassion Training (CBCT) for Breast Cancer Survivors: A Randomized, Wait List Controlled Pilot Study.” Supportive Care in Cancer: Official Journal of the Multinational Association of Supportive Care in Cancer 23 (12): 3599–3608. https://doi.org/10.1007/s00520-015-2888-1.
Lang, Ariel J., Anne L. Malaktaris, Pollyanna Casmar, Selena A. Baca, Shahrokh Golshan, Timothy Harrison, and Lobsang Negi. 2019. “Compassion Meditation for Posttraumatic Stress Disorder in Veterans: A Randomized Proof of Concept Study.” Journal of Traumatic Stress 32 (2): 299–309. https://doi.org/10.1002/jts.22397.
LoParo, Devon, Sallie A. Mack, Bobbi Patterson, Lobsang Tenzin Negi, and Nadine J. Kaslow. 2018. “The Efficacy of Cognitively-Based Compassion Training for African American Suicide Attempters.” Mindfulness 9 (6): 1941–54. https://doi.org/10.1007/s12671-018-0940-1.
Pace, T., L. Negi, B. Donaldson-Lavelle, B. Ozawa-de Silva, S. Reddy, S. Cole, L. Craighead, and C. Raison. 2012. “P02.119. Cognitively-Based Compassion Training Reduces Peripheral Inflammation in Adolescents in Foster Care with High Rates of Early Life Adversity.” BMC Complementary and Alternative Medicine 12 (1): P175. https://doi.org/10.1186/1472-6882-12-S1-P175.
Reddy, Sheethal D., Lobsang Tenzin Negi, Brooke Dodson-Lavelle, Brendan Ozawa-de Silva, Thaddeus W. W. Pace, Steve P. Cole, Charles L. Raison, and Linda W. Craighead. 2013. “Cognitive-Based Compassion Training: A Promising Prevention Strategy for At-Risk Adolescents.” Journal of Child and Family Studies 22 (2): 219–30. https://doi.org/10.1007/s10826-012-9571-7.
“Twelve lines of dialogue,” “two and a half hours of runtime,” “world’s saddest flirting,” and “Academy Award-winning glance choreography.” These are some of the similarities SNL found between Portrait of a Lady on Fire (2019) and Ammonite (2020) in their fictional trailer called “Lesbian Period Drama.” In this skit, SNL highlighted the apparent trend in queer filmmaking that restricts lesbian narratives to the 18th century.
SNL’s “Lesbian Period Drama” trailer.
Though SNL was just trying to be funny, “glance choreography” is an aspect of the critical concept that I call the queer lens.
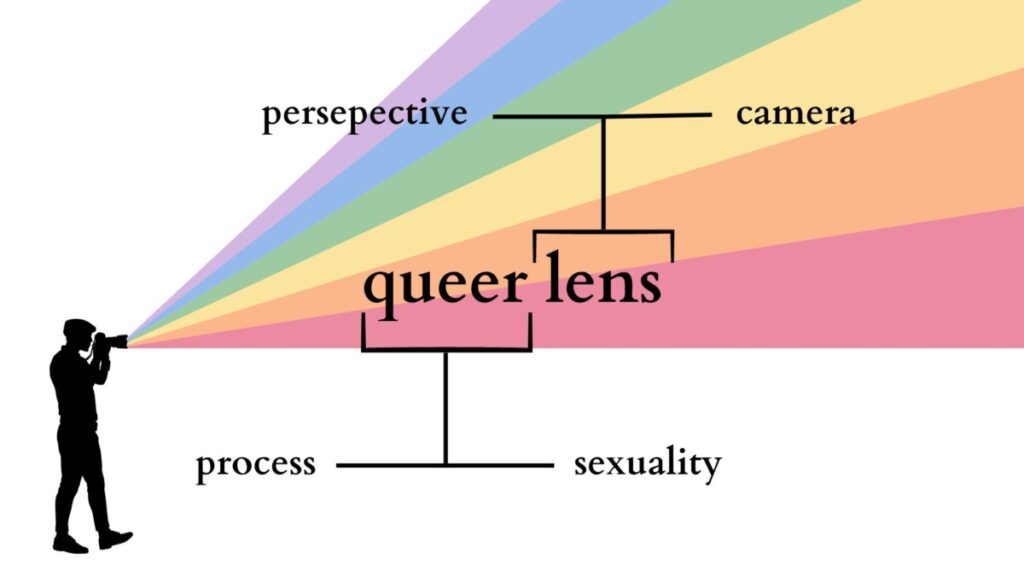
There are numerous theorists who specialize in the study of the “glance” in cinema, or more specifically the gaze, notably Laura Mulvey, Jacques Lacan, and bell hooks. Filmic gazes, however, emphasize spectatorship and the inherent power dynamics within. Rather than focusing on spectatorship theoretically, I think it more fitting to consider the role of the camera that singles out the hidden details that fuel queer tension and desire, the details found most often in the form of these looks and gazes. That’s why I call it the queer lens; the duality of the “lens” serving as one of the camera’s and as one of a perspective (Fig. 1).
Fig. 1. A schematic of the queer lens and the various aspects explored within the concept.
In this blog, I will take you through a little journey of how the queer lens works in the filmmaking world with Céline Sciamma’s 2019 Cannes Best Screenplay-winning film, Portrait of a Lady on Fire, as our case study.
To start off with a brief summary, Portrait is set on an island in Brittany, France, in 1770. The film is about a painter, Marianne (Noémie Merlant), who is commissioned to paint a wedding portrait of Héloïse (Adèle Haenel), a reluctant bride-to-be who has just left the convent. Due to Héloïse’s resistance for the marriage and subsequent refusal to sit for a portrait, Marianne must do so without her knowing. She observes her carefully by day, acting as a companion on Héloïse’s walks so she does not follow the same fate as her deceased sister, and painting her secretly.
The women in Portrait engage in an equal, reciprocal relationship, favoring feminine ways of looking that is often negated in hegemonic, patriarchal narratives and ways of looking. The queer lens allows such looking amidst oppressive environments through the use intentional cinematography. Let’s take a look at how Sciamma and her director of photography, Claire Mathon, made this work.
Marianne’s POV Shots
Throughout the beginning of the film, Marianne and Héloïse’s walks consist of close shots of Heloise’s face from behind, so as to show Marianne’s point of view trailing behind her. The fact that Marianne cannot get ahead of Heloise subtly hints at the difficulty Marianne encounters with memorizing Héloïse’s face to paint later at night by candlelight or in the morning. But perhaps more importantly, the fact that Héloïse is always ahead opens the possible interpretations for the several seemingly furtive glances towards Marianne – is Héloïse curious? Scared? Suspicious? Maybe even interested? The fluidity of such an aesthetic mirrors the fluidity of queerness itself, both in its ever-changing meaning in academia and its fluctuation of sexuality (Fig. 2).
Fig. 2. Héloïse turns to look back at Marianne, almost breaking the fourth wall given Marianne’s POV shot.
A Look is Worth a Thousand Words
Even when the two sit next to each other – a tight medium close-up shot’s distance apart – Marianne can’t just turn and stare at Héloïse discreetly without drawing suspicion to her real mission (Fig. 3). In some ways, however, the consistency of such glances and gazes contribute to the underlying, budding connection and desire between the two women. The tightness of the shot forces Marianne and Héloïse’s proximity much closer together than one might expect between two women who had just met, especially in the 18th century. Every time this occurs, they hardly break eye contact and look each other up and down carefully; Marianne perhaps because it’s her job and Héloïse perhaps due to her continued curiosity or interest.
It is the queer lens that offers this perspective in a world where the women can transport out of the restrictive reality and destinies they are bound to. The camera’s lens is queered in the looks rather than the dialogue, as “what remains unsaid remains most poignant” and most illuminative. SNL’s joke about the “twelve lines of dialogue” in the “two and a half hours of runtime,” though exaggerated, hints at exactly these looks that do all the talking to promote the growing attraction between the women. Consider this: queer during this time period meant “strange or eccentric,” so it’s not like Héloïse really had the option to ask Marianne, “Wait, are you queer?” It’s the camera’s role in the queer lens to consider this question in-explicitly.
Fig. 3. Tight medium close-up shot of Héloïse (left) and Marianne (right) delicately looking at each other. The queer lens illustrates the simmering tension and desire amidst their oppressive environment.
Transformative Shot-Counter Shots
After Marianne reveals her true purpose to Héloïse, showing her the first rendition of the portrait, Héloïse resents Marianne’s failure to really see her and capture her vitality (“Is that me? Is that how you see me?”). I interpret this narrative development to suggest that Héloïse had sensed an attraction growing between them – as made evident from the looks leading up to this moment – but now wishes to be seen for who she really is, more so by Marianne than by the Milanese gentlemen whom she is predestined to marry. This inspires a collaboration between the women, as this time Héloïse agrees to sit for Marianne’s painting.
Mathon uses conventional shot-counter shot composition with a focus on medium close-up shot variations to govern the love relations fueled by looking in these moments that the women collaborate for the painting. She does so in a new, transformative way that bridges the gap between the painter and the muse. It becomes evident that the sexual attraction that the queer lens builds is not built on domination or ownership; rather, it is “grounded in mutuality and understanding.”
Fig. 4. Marianne paints Héloïse’s portrait, glancing at her carefully by the nature of the art. The queer lens flourishes as a result of Marianne’s painting, masked as strictly an occupation with hidden layers of desire.
Additionally, it’s important to acknowledge the considerable amount of time, energy, and most importantly, looking required for drawing, sketching, and painting (Fig. 4). So it’s one thing that Marianne sketches Héloïse sleeping later at night, but it’s another thing when Héloïse wakes up to notice her, and they inevitably share a gaze and a smile. To capture someone’s presence and vitality on a piece of art is to not just see them, but to understand them – something Marianne achieves better than perhaps the future male recipient of the portrait ever will.
Queering the Period Drama Setting
The 18th century setting wherein Portrait takes place inherently incorporates motifs often associated with romance, such as low lighting coming from natural sources like candles and a fireplace that warm up the atmosphere when Marianne sketches Héloïse. As Mathon said in IndieWire’s Filmmaker Tookit podcast, “[Céline Sciamma and I] were talking about re-inventing and enhancing our 18th century image to current realities.” I interpret this as the film not just showing a painter painting, but it becomes a painting (Fig. 5). There is an abundance of softness, both in terms of the lack of hard shadows and the texture of the actors’ skin suggesting that of an oil painting. “We often discussed the faces in terms of the landscapes,” Mathon mentioned, elaborating on the detailed and heightened color choices.
Fig. 5. The natural, soft lighting of the fireplace illuminates the dinner scene with Héloïse, Marianne, and the maid Sophie (Luàna Bajrami), from left to right.
Sciamma and Mathon’s meaningful choices in the mise-en-scène – a term for everything in front of the camera, from costumes and make-up to lighting and blocking – transports us to this reinvented, queered 18th century reality where the once illegal and unacceptable desires are allowed to exist. Echoing the nature of the queer looks necessary for painting the portraits, the painting-like nature of the environment queers the 18th century setting. This offers Marianne and Héloïse a space for agency to navigate their lives that they perhaps would not have found otherwise – at least for a couple weeks before the patriarchy inevitably reminds them of the reality they live in. As depressing as it is to consider the parting between the women, would it really be realistic to have a happy-ever-after ending given the 18th century conditions for queers? Unfortunately yet pragmatically, I think not.
So despite SNL calling Marianne and Héloïse’s budding romance “the world’s saddest flirting,” we are left feeling love and despair for their circumstances. The multifaceted dimensions of the queer lens guides our eyes and hearts to understand queer desire with a new perspective, even when queer cinema shifts to lesbian period drama trends.
So, you’re pregnant. Congratulations! No doubt, you already have a ton of questions running through your head— What’s so great about the new $1,200 Nuna stroller? How many diapers is too many? Is co-sleeping REALLY that bad (it’s just cuddling on steroids, right…)? These are all exciting topics to dive into as you prepare for the next great addition to your family. But if you’re having a boy, there might be one question on your mind that seems a little more daunting and a little less exciting to have to deal with: What the heck should you do about his foreskin?!
In this post, I’ll give you all the information you need about circumcision—anatomy, history, medical effects, and cultural considerations—in as factual and straightforward a manner as possible, so you can get back to stroller shopping in no time.
Male circumcision is a surgical procedure that removes the foreskin (retractable piece of skin) from the head of the penis.
On average, the skin that’s removed contains more than 3 feet of veins, arteries, and capillaries, as well as about 20,000 nerve endings.
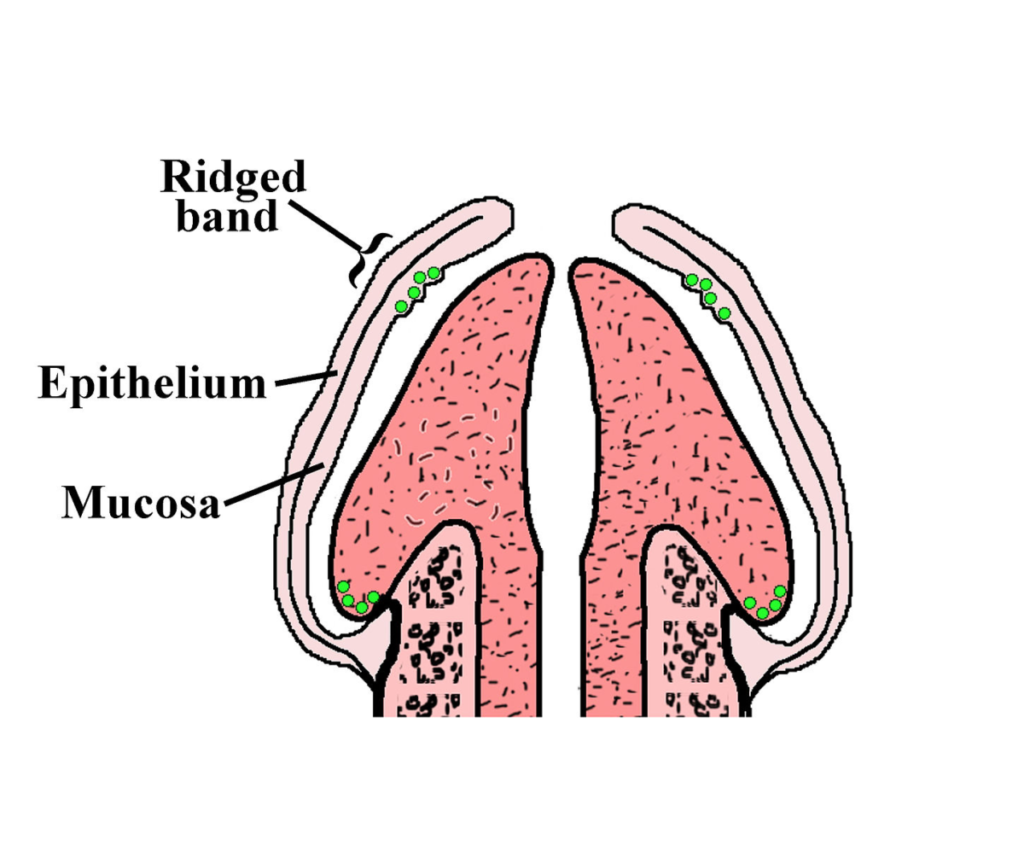
Foreskin contains the “ridged band”— the heavily innervated mucosal tissue that’s intended to provide natural lubrication during sexual arousal.
Foreskin protects the head of the penis from friction against clothes. This is important because constant friction can reduce sensitivity, therefore reducing sexual pleasure.
There’s no clear line of demarcation between the foreskin and the rest of the skin on the shaft penis. This means that there’s no set amount of skin that can or should be removed during a circumcision– the amount that’s removed varies depending on where and by whom the procedure is performed.
Summary: The foreskin is made up of very sensitive tissue that serves a unique purpose in sexual functioning.
Anthropologists believe that male circumcision could date as far back as 2,300 BCE, to Old Kingdom Ancient Egypt. Since then, it acquired ritualistic value in cultures ranging from Judaism and Islam to tribal Polynesia. In the 1870s, it regained popularity after a few American pediatricians made claims that it cures paralysis and prevents masturbation—which, at the time, was thought to be a great sin, a sign of mental weakness, and the cause of serious illness and death. Though it is not true that the procedure prevents masturbation, more modern science has shown that circumcision can actually have some medical benefits. Let’s take a closer look at those.
It’s well-established that circumcised men are less likely to acquire and transfer HIV under certain circumstances. Such circumstances include lacking access to healthcare, condoms, or soap and water.
In developed countries such as the United States, circumcision is not an effective preventative tool for HIV/AIDs or other sexually transmitted infections. A far better option would be regular washing and use of condoms.
Penile cancer:
Penile cancer is extremely rare, effecting fewer than 1 in 100,000 men each year (0.001%).
Evidence shows that a higher proportion of men with penile cancer are uncircumcised. However, this correlation is believed to be the result of a rare condition called phimosis, which can be prevented through regular washing, and treated with circumcision on an as-needed basis later in life, if necessary.
In the United States, the average age of onset for penile cancer is about 60 years old. Some other (likely more effective) preventative measures include regular washing of the penis, and abstaining from smoking.
Urinary tract infections:
In 2012, the American Association of Pediatrics released a policy report stating that in their view, the benefits of circumcision were worth the risks, citing UTI prevention as their primary reason. However, this report received heavy academic criticism for misrepresenting data, and it expired without ever being renewed.
UTIs are very rare in males, and virtually never occur after the age of two. In contrast, they are very common in women of all ages—at least every other female will get a UTI during her lifetime.
Approximately 100 circumcisions would be needed in order to prevent a single boy from acquiring one UTI.
UTIs are very easily treated with a few days of common antibiotics.
Summary: While HIV, penile cancer, and UTIs are statistically significant correlates of circumcision, this does not lead circumcised boys to have better overall health outcomes in the United States.
Circumcision is usually a quick and safe procedure, though serious complications such as infection arise about 1% of the time.
Circumcision is a painful procedure, both in the moment and during the healing process. Healing takes about one to two weeks. Local anesthesia should always be used to minimize pain.
As a boy grows, so will the surface area of his skin. Sometimes the new skin naturally ends up growing back to a length that can retract, leading parents and pediatricians to want to give their boys circumcision “revision” procedures a few years after the initial procedure. While most American insurance companies cover an initial circumcision, most do not cover revisions.
Circumcision removes a unique structure which contains heavily innervated skin and mucosal tissue, and also protects the glans from excessive friction against clothing. As a result, some research has shown that circumcised men and their partners may experience less sexual pleasure than uncircumcised men and their partners.
Some circumcised men report that erections, sex, and masturbation are more painful due to a lack of skin, which can cause a feeling of “tightness” and curvature of the penis.
Summary: Circumcision usually does not lead to serious medical complications, but it may lead to decreased sexual pleasure and increased risk of pain from sexual arousal and activity.
Though virtually every American-born male was circumcised soon after birth in the mid 20th century, in recent decades the practice has seen a significant decrease in prevalence. Some states still practice it relatively frequently, but in some states, only 10% of boys are circumcised at birth.
Since the procedure is not medically necessary, potentially harmful, is conducted on people who cannot consent, and interferes with very intimate body parts and functions, many scholars consider circumcision to violate the principles of bioethics.
Most other wealthy countries no longer practice male circumcision routinely, and some have made it illegal. In America, too, it’s illegal to perform any genital alteration on female infants, even in ways that are far less invasive than our typical male circumcisions.
A 2018 study showed that on average, circumcised and uncircumcised men are equally satisfied with their circumcision statuses. However, false beliefs about the practice can impact people’s satisfaction levels.
Studies show that people’s preferences for circumcised vs uncircumcised sexual partners vary greatly depending on their sexual orientation, past experiences, and where they live.
Summary: Though infant circumcision is still somewhat of a standard in American culture, people’s preferences for it vary greatly across the country, and it receives strong criticism from both American scholars and the general public in most other developed countries.
—
So, do with this information what you will, and go get back to stroller shopping!

















{kind=link}