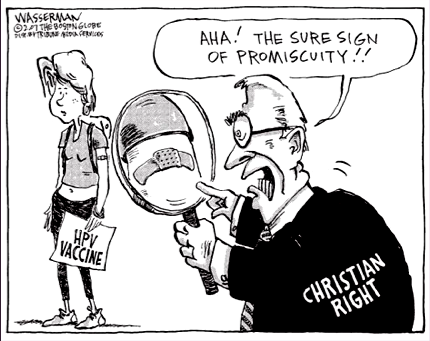
So far this semester, we have addressed the means by which AIDS and STI’s are spread and the facility of women to contract these diseases. Not only does biology appoint women as easy contractors of AIDS but their vulnerability through sexual violence also makes them optimal contractors of this disease. Gay males too carry the stigma for being HIV positive because of their sexual preference and for some, their promiscuity. [1] “From 1981, AIDS was firmly constructed into the west as a disease affecting male bodies, more specifically the bodies of gay men (Richardson, 127).”
Whether these two groups contribute largely to the HIV positive community however, we have not addressed another population of HIV positive individuals who are neither women nor gay men- heterosexual male prostitutes. Don’t be fooled into thinking that all male prostitutes are gay or non-heterosexual and only service women. These are false assumptions.
[1] “Sexualizing the HIV-infected body as gay also encouraged the view that heterosexual men were also not at risk and, by implication, “safe” (Richardson, 128). Although AIDS has been firmly constructed as a ‘male disease’ in the west, the heterosexual male is largely invisible in AIDS discourse (Richardson, 138).”
Curious to find more info about these individuals who linger the streets afterhours, I came upon a short documentary for a new campaign named Invisible: The Unseen World of Male Prostitution. This documentary focuses in on the struggles of male prostitution in Rhode Island. Whether this documentary is fictional or not, does not deviate the focus for new groups that are affected by AIDS; as we tend to focus more on women and gay men prevention.
[2] What this documentary does reveal is the lives of male prostitutes who roam the streets picking up ‘tricks’ for a couple bucks in order to feed their drug addiction. Surprising too, is that they are not all (not seemingly) gay men. They describe the necessity to work the streets in order to acquire the drugs that they need and sometimes having 8-10 clients per night. One male prostitute discusses the lack of AIDS fear and how there are those men who admit their probability of AIDS contraction however, that this does not affect the number of ‘tricks’ they pick up. These heterosexual males have families, girlfriends and are NOT GAY and to put it simply, they are doing what they gotta do to get their fix. It is important to realize that we as a community focus too much on stereotypes and stigma and assume that all who are HIV positive are victims of rape and gay men, why must the stigma stop there?
As discussed in class, we generally think that AIDS prevention entails safe sex with condoms and educating others of AIDS. If everyone is educated, will AIDS stop? What I gathered from this video is that these men are aware of AIDS but there is no real fear for contracting the disease nor spreading it. They just want their drugs and unprotected sex guarantees them more money for their addiction. If then, they know about AIDS and the means of contraction then would further education really make a difference to the spread of AIDS? This is the big question here. What, if any, amount of education is really needed to teach the public about AIDS contraction so that everyone will commit to safer sex practices? In her article, “Structural Violence, Poverty and the AIDS Pandemic”, Jola Mukherjee writes that it is reasoned that AIDS can be prevented through behavior change.
[3] “HIV prevention can be viewed as two interrelated entities: risk avoidance such as abstaining from sex and drug use; and harm reduction that is minimizing risk while conduction behaviors that are associated with HIV (use of clean needles for drug users and use of condoms). Prevention is often presented as “life-style choices…yet those who live in poverty have severely constrained choice (379).”
If poverty then, is a major factor of AIDS contraction, how can these men who are already struggling to make ends meet, have the opportunity to get the help they need. It is easy for us to reason that their safety is just a trip to Rehab away. This may be an easy solution however, if they chose to leave the streets, where will they find the funds to pay for rehab? If they decide one day that they want to leave the streets, how will they find a job? Who would want to hire them? Are those who continue to have unprotected sex and continue to contract others morally wrong for doing this? Do they feel no obligation to protect others and their well-being just as no one seems to care about their own well-being?
What we need to gather from this documentary and these articles is that, AIDS is not discriminatory. All colors, cultures, and genders are vulnerable to AIDS so we must not aim AIDS support to only specific communities. We must revise our plan of action and find new solutions to help those in need while protecting ourselves from this epidemic.
[1] Richardson, Diane. “In/Visible Women and Dis/appearing Men.” Rethinking Sexuality, 127-138.
[2] KickStarter.com. Invisible: The Unseen World of Male Prostitution. 29 Oct. 2012. Web. 7. Nov. 2012 <http://www.kickstarter.com/projects/1928510921/invisible-1>
[3] Mukherjee, Joia S. “Structural Violence, Poverty, and the AIDS Pandemic”. Sexual Disease, 379-385.