
This case Courtesy of David Zhou and Patrick Meloy:
EMory Files
Case #7: Deltoid Abscess
Hx: 37 yo female with a hx of IV heroin abuse (IVDA) who presents with bilateral shoulder pain. She has been injecting heroin using the skin popping method
PE: Temp: 37.3 °C, Heart Rate: 60, RR: 17, BP: 122/58 mmHg, SpO2: 100 %. Fluctuance in bilateral shoulders’
Complications of IVDA:
Teaching Point #1: Deltoid abscesses require careful evaluation and drainage due to the high risk of bleeding and deep tissue involvement
Teaching Point #2: Admit and antibiotics all IVDA’s with fever
Teaching Point #3: In addition to soft tissue infections, IVDA’s are at risk of other serious infections
Clinically Focused Review Article:
William T. Hosek, John Gullett, Adult Female With Shoulder Pain, Annals of Emergency Medicine, Volume 55, Issue 1, January 2010, Pages e1-e2, ISSN 0196-0644, http://dx.doi.org/10.1016/j.annemergmed.2009.08.009.
(http://www.sciencedirect.com/science/article/pii/S0196064409014346)
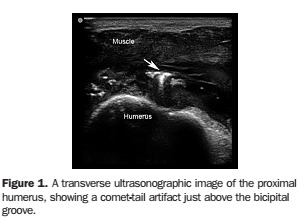
1. How do I evaluate and treat a deltoid abscess? Think twice about draining these in the ED. Deltoid abscesses are more likely to require operating room drainage due to deeper infections with higher chance of developing necrotizing fasciitis and bleeding complications. Ultrasound and CT imaging can be used to evaluate depth and involvement of surrounding tissue. On US: abscess appears anechoic and soft tissue gas generates comet tails. Abscesses can also contain needle fragments. Note important surrounding anatomic structures.
2. What to do about an IVDA with fever? ADMIT and Broad Spectrum Antibiotics! Infections such as endocarditis cannot be ruled out in the ED. Cardiology should be aware for TTE & TEE as inpatients. Drug use within 5 days, fever greater than 102 F and proteinuria have been found to be useful predictors of admission. Other IVDA sources of fever: hepatitis, skin and soft tissue infections, tetanus, septic arthritis and osteomyelitis, pulmonary infections, endophthalmitis, meningitis, and epidural abscess and brain abscess
3. What about spinal epidural abscess (SEA)? IVDA increases risk of SEA. Staph in addition to gram-negative rods are possible in IVDA. Presentation: fever, back pain, neuro deficit. PE: urinary retention, localized back tenderness, motor and sensory deficits, positive straight leg raise and saddle anesthesia. Workup: blood cultures, CBC, ESR, and gadolinium enhanced MRI (CT myelography can be used as an alternative to MRI if needed). Treatment includes antibiotics (vancomycin with cefepime initially), infectious disease consultation and likely surgical drainage with associated laminectomy. Timely identification and treatment is key to a good prognosis in terms of neurological sequelae.
4. What about endocarditis? Dukes Major and Minor Criteria. + Cultures/fever/murmur. TTE and TEE are critical. Empiric antibiotics until organism isolated. Antibiotic and surgical treatment guidelines available at: European Society for Cardiology Guidelines.
Case Resolution:
Surgery consult. Drained in ED by Surgery . Vanc IV observed in the CDU and discharged on PO Bactri