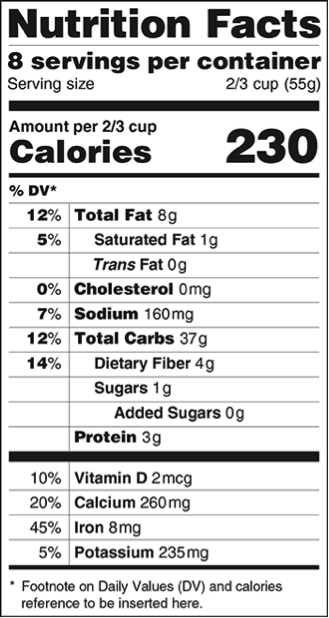
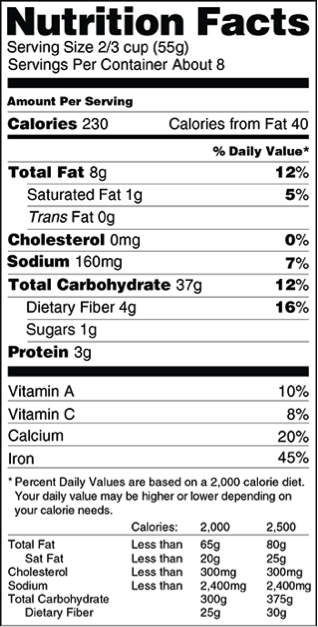
In the article discussing public health initiatives to combat obesity and their ethicality, Holm argues that there are three different forms of paternalism: hard paternalism (direct coercion), soft paternalism (giving unwanted information or foreclosing some options for action), and maternalism (control by inducing a guilty conscience). He then applies these types of paternalism to a discussion of the ethics behind obesity interventions. The first question is whether it is justifiable to promote a person’s own health or well-being, if they do not want intervention. I immediately thought of the ethicality of posting calorie counts at restaurants. If the person does not want the information, this is most definitely a form of soft paternalism, and even a little bit of maternalism as guilt may prevent someone from ordering what they want. But is it justified?
Recent Studies
Recent studies have found that while an estimated 15% of restaurant customers used calorie listings to help them choose healthier foods, the majority of listings were too confusing to guide diners to make healthier decisions. Programs like these often encourage businesses to work towards putting healthier and more nutritious items on their menus as they know that customers will be provided with the nutritional facts in an easy and convenient way. For example, it is embarrassing for McDonald’s to have to disclose that 20 Chicken McNuggets is 860 calories. Thus this provides both an incentive for business owners to provide healthier alternatives as well for consumers to make healthier eating decisions.
Autonomous Decision Making
Misinformation, along with busy lifestyles and too many unhealthy choices, has been pegged as one of the leading causes of the obesity epidemic. In order for consumers to make a fully autonomous decision based on informed choices, they must have enough information to do so. While it is likely that the calorie listings encourage people to make healthier decisions, the information provided is in no way biased. The calorie listings are simply stating the facts and thus I don’t think it is fair to view them as a bias or a source of forced paternalism. I think the main question is whether or not society or the state is justified in interfering in our personal choices. But is it really interfering if they are only helping us make a more well informed decision? I argue that no. The displays of calorie values are ethical as well as important to the health of our society. There is no loss of freedom or autonomy in being provided the extra information, in fact autonomy is actually increased as more information allows one to form a better informed decision.