
A 39 year-old female with current medical history of cocaine abuse and uterine fibroids reports to the ED with 2 days of abdominal pain. The pain was sudden in onset, sharp, and severe. It has progressed in severity over the past two days. The pain was initially in the lower abdomen, but is now diffuse. The pain is worsened by movement, with no alleviating factors. The pain did have a temporal relation to cocaine use. The patient has experienced no other symptoms, such as nausea, vomiting, dysuria, or bleeding.
Physical exam is significant for rebound tenderness on abdominal and pelvic palpation and percussion. The pelvic exam is remarkable for a 36 week gravid-sized uterus, which the patient states is unchanged as compared to her pre-event state.
Labs are significant for a WBC count of 14.1, lactic acid of 7, and a H/H of 7/21. Previous labs in the system show H/H of 14/42. Pregnancy test is negative. The patient was actively resuscitated with blood and crystalloid, and a surgical consult was requested.
CT scan of the abdomen and pelvis reveals massive quantities of free fluid with radiographic densities concerning for layered blood, especially around four profound uterine fibroids. No free air is detected.
The patient is taken emergently to the OR by the OB/GYN service for TAH/BSO. The patient is found to have multiple degenerating fibroids, all of which are bleeding intraperitoneally. Estimated blood loss is nearly two liters.
After three days, the patient is discharged with no further complications.
Spontaneous hemoperitoneum has been reported from a variety of conditions, including hepatic, splenic, vascular, and gynecologic sources. Regions of high attenuation in a peritoneal hematoma (signifying older, proteinaceous, clotted blood) may give clues as to the origins of the bleeding. Active bleeding (contrast blush) seen on CT mandate immediate surgical or interventional procedures. Unlike some cases of traumatic hemoperitoneum, which can be managed by observation, non-traumatic hemoperitoneum almost always mandates exploration.
Uterine fibroids are rarely a cause of hemoperitoneum. There have been approximately 50 cases described in the literature in the past 50 years. There is no description in the literature of hemoperitoneum from multiple uterine fibroid rupture, as seen in this patient.
The temporal relation of the patient’s condition to her cocaine use raised considerable alarm. Cocaine abuse has been linked as an independent risk factor for hemoperitoneum and other abdominal catastrophes. Of particular note, cocaine is notorious for an association with duodenal and juxtapyloric ulcer perforation. Dr. David Feliciano, former head of Grady’s department of surgery, described a case series of 50 patients with this injury over a decade. Most concerning, nearly a quarter of patients with this type of perforated ulcer do not demonstrate free intraperitoneal air. Cocaine has also been linked to mesenteric ischemia and bowel infarction. Overall, a very high index of suspicion for abdominal catastrophe should be maintained for patients with abdominal pain in the setting of cocaine use.
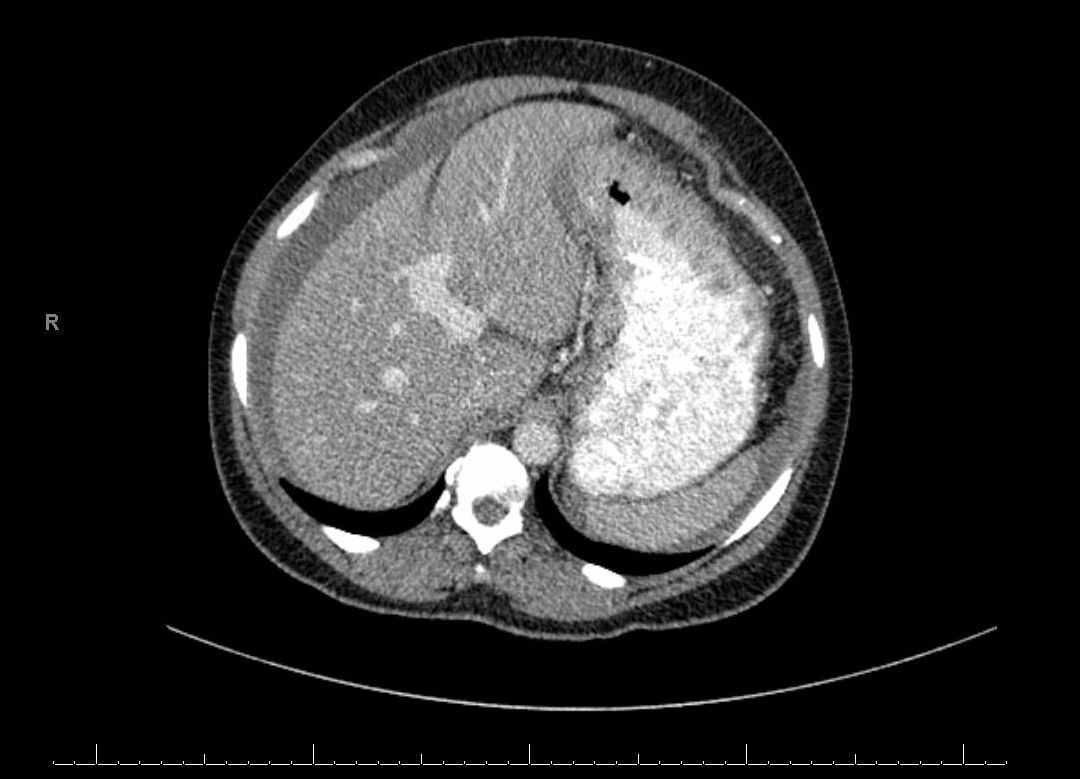
Note fluid collection along the edge of the liver — hemoperitoneum
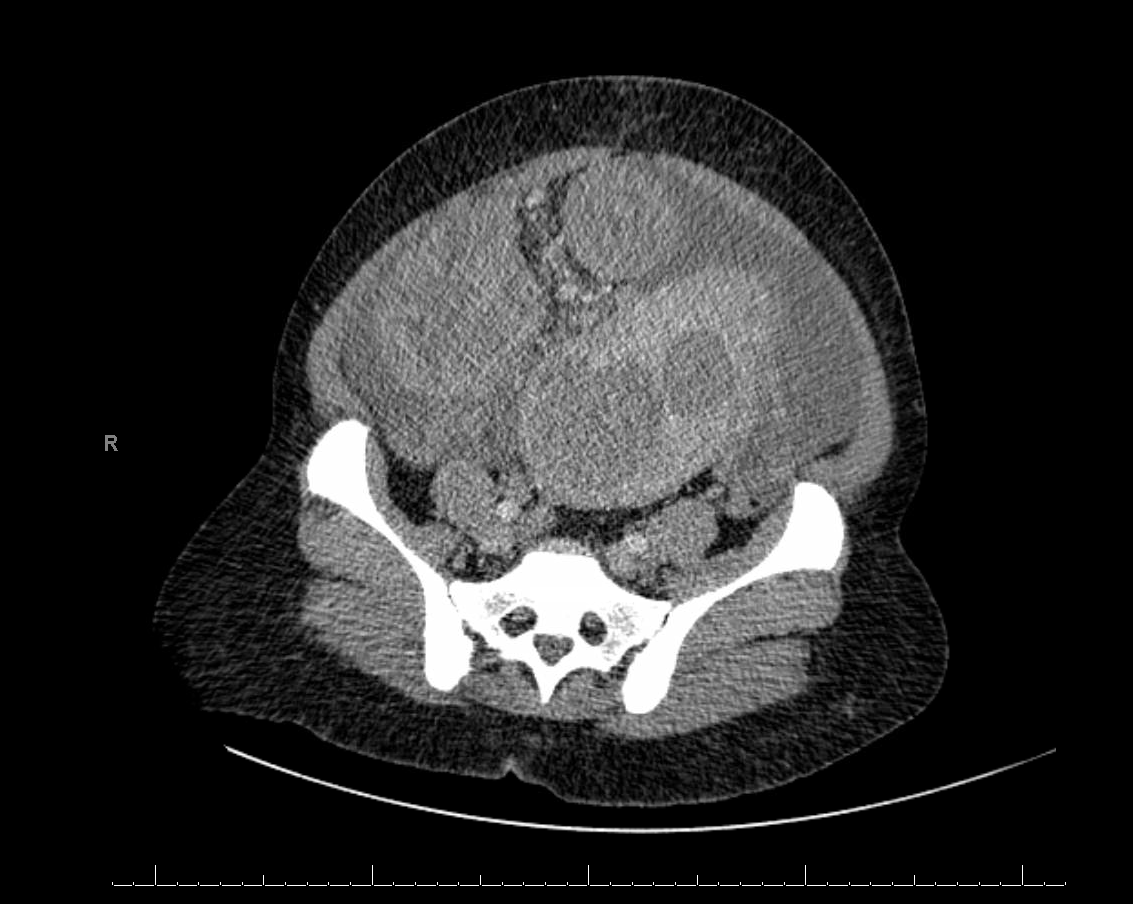
Higher density clotted blood surrounds missive fibroids, giving a clue as to the origin of the patient’s condition
Article 1. Spontaneous Hemoperitoneum Non-GYN
Article 2. CT Findings of Hemoperitoneum
Article 3. Cocaine and Spontaneous Hemoperitoneum
Article 4. Perforated Juxtapyloric Ulcer and Cocaine Use — Feliciano
Article 5. Hemoperitoneum Secondary to Uterine Fibroid