
The ADJUST PE trial is hot off the JAMA presses in March 2014. The takehome: of 1141 patients excluded from scanning by clinical assessment plus age adjusted d-dimer, there were only 2 cases of non-fatal PE (0.2%). Of these 1141 patients, 331 had an age adjusted d-dimer greater than the standard cutoff of 500mg/mL. Of these …
Tag: PE
Jun 07
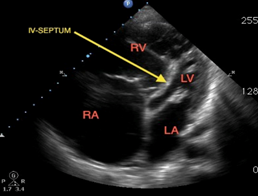
CHF or PE? PE is a known and common complication of CHF
challenging case: an obese 60yo patient never seen by a doctor as an adult presents marked peripheral edema, hypertension, and 2 months of worsening DOE, PND, orthopnea. BNP 400, EKG Unremarkable, trop 0.1, stating well. It feels like CHF. But the cardiologist wants a CTPE. We oblige – big saddle embolus with RV strain. This …
Jun 06
How to give thrombolytics
[notice]PHARMACOLOGY[/notice] A great question came up in the zones. We see and likely should be comfortable with the dosing of Alteplase for CVA. Grady is a renowned Stroke Center and I would certainly have any of my family members come to the Marcus Stroke and Neuroscience Center if they were having a stroke. The fact …
Jun 04
Finger Thoracostomies
From teaching round–Courtesy of Mene Demestihas: In a patient in cardiopulmonary arrest, going through the H’s and T’s can lead us to suspect a tamponade or compressive physiology as the culprit of the arrest. In these patients placing a formal chest tube is generally frowned upon as it can be a labor-intensive process for a …
May 13
Case of the Month #5
EMory Files Case #5: Massive PE Hx: 40 yo F hx of Lupus presents with CP SOB PE: VS: BP 90/50, HR 125, RR 30, O2 88%, afebrile. Awake and alert, mild distress improved with nonrebreather. Case Discussion Massive PE: ***Case Discussion Wissam Jaber, Dir. PE Response Team*** https://www.dropbox.com/s/9xv0iqg5f4p9a0e/PE%20Jaber%20Interview.mp3 Teaching Point #1: Negative …