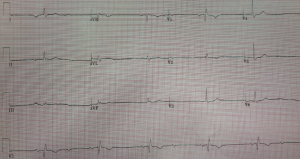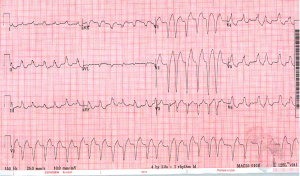
A 60 yo male came into Midtown a few days ago for generalized weakness. He was hemodynamically stable and the EKG above was obtained. With an irregularly irregular wide complex tachycardia like this our differential is fairly short… 1) A-fib or MAT with aberrant conduction (aka a bundle branch block) 2) A-fib or …