
EM Journal Club Reviewer: Jason Holmes Article Rapid Blood-Pressure Lowering in Patients with Acute Intracerebral Hemorrhage Craig S. Anderson, M.D., Ph.D., Emma Heeley, Ph.D., Yining Huang, M.D., Jiguang Wang, M.D., Christian Stapf, M.D., Candice Delcourt, M.D., Richard Lindley, M.D., Thompson Robinson, M.D., Pablo Lavados, M.D., M.P.H., Bruce Neal, M.D., Ph.D., Jun Hata, M.D., Ph.D., Hisatomi …
Jun 25
When a sore throat is more than just a sore throat…

This is a patient that I saw in the ED a few weeks back. She was a young otherwise health female who presented to the ER for several days of sore throat, pain with swallowing, and difficulty swallowing. On exam her airway was patent and she did not have stridor. She had tenderness over the anterior …
Jun 24
Playing tennis and you feel a pop?
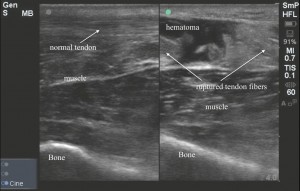
The IOW this week comes from Dr. Nicole Franks. Her patient is 48 year old male, who presented to the ER with ankle pain and difficulty with ambulation after an injury while playing tennis. He reports he heard a pop when the injury occurred. Bedside ultrasound above was obtained. To get this image place the patient …
Jun 20
Hip Pain and Negative Plain Films

Case: A young person presented following an MVC. Initial workup was negative including plain films of the chest and pelvis, however the patient had some tenderness over the right greater trochanter, and some pain with passive ROM, limiting movement overall. On tertiary exam in the ED, the patient was unable to bear weight on the …
Jun 20
Spontaneous Hemoperitoneum
A 39 year-old female with current medical history of cocaine abuse and uterine fibroids reports to the ED with 2 days of abdominal pain. The pain was sudden in onset, sharp, and severe. It has progressed in severity over the past two days. The pain was initially in the lower abdomen, but is now diffuse. …
Jun 19
Master the BVM
Why is it important to be proficient with the BVM? Because inevitably we will all have patients that are difficult to intubate, but if we can ventilate these patients with the BVM we can buy ourselves time to use our alternative techniques. If you can’t ventilate effectively with the BVM you find yourself in a …
Jun 18
To shock or not to shock that is the question?
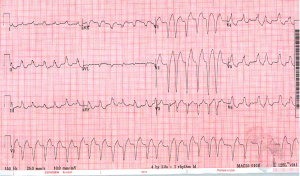
A 60 yo male came into Midtown a few days ago for generalized weakness. He was hemodynamically stable and the EKG above was obtained. With an irregularly irregular wide complex tachycardia like this our differential is fairly short… 1) A-fib or MAT with aberrant conduction (aka a bundle branch block) 2) A-fib or …
Jun 15
Followup on Dr. Pendley’s Nailbed Post

This is a piece of suture foil that is used to repair a partial nail avulsion. Remember, you can use non adherent gauze or suture foil to lift the nail fold off of the nail bed.
Jun 14
In patients with partial nail avulsion with preserved nail structure, and without laceration or fracture, should I remove the nail?

No: the remaining nail acts as a protective splint for the underlying nail bed and holds the nail fold open, which may take 60-170 days. Use a digital block followed by copious betadine/water and soak the hand. Explore the margins, find the intact nail fold and reapproximate the nail. You may also need to explore …
Jun 13
DKA and HHS
HHS v. DKA: 1) What’s the difference? HHS patients, as opposed to DKA patients, usually have some residual circulating insulin that prevents secretion of glucagon and glucocorticoids. These hormones are responsible for the breakdown of free fatty acids and the formation of ketone bodies seen in DKA. 2) What about this patients …