While homicide rates in major cities across the country fell in 2013, Atlanta’s rate remained much the same. There were 84 homicides in the City of Atlanta during 2013, as compared to 83 in 2012, according to the FBI Uniformed Crime Report.
According to the report, 72 men and 12 women were killed. Of those killed, 72 were African-American, 10 were white, one was Asian, and the other was unknown. Victims were killed overwhelmingly by a stranger with a gun.
Below is a timeline of the murders, with a description of what the police believe happened, according to police reports. Additionally, there is a map of where the murders occurred.
“How many people in this crowd have seen Molly?” Madonna asked the audience at Ultra Music Festival in Miami in 2012 when she was introducing the popular DJ Aviccii.
She said she was referencing the song “Have You Seen Molly?” by Cedric Gervais. But most people in the crowd assumed she was referencing the drug Molly, which has become prevalent at music festivals around the country.
College senior Sarah, who asked to use a pseudonym for purposes of this article, was first introduced to the drug two years ago at Day Glow, the world’s largest paint party featuring electronic dance music.
“People kept coming up to me asking ‘oh do you know Molly?’” Sarah says. “And I was like, ‘who is this girl? She sounds really popular.’”
She is really popular.
Sarah took her first MDMA pill at an electronic dance music concert one year later and didn’t feel much. The next weekend she took two pills. Five days later she lost feeling in her legs, had a panic attack and was taken to the hospital.
Sarah is just one of many college students experimenting with Molly.
The Drug Enforcement Agency classifies Molly as the powder or crystal form of MDMA, the chemical drug most commonly known as the main ingredient in Ecstasy. Defined by users as a “pure” form of MDMA, its fans consider Molly safe, unlike Ecstasy, which has a reputation of being laced with anything from fertilizer to methamphetamine. But, according to the DEA, Molly is a Schedule 1 controlled substance with high possibility for abuse and addiction and no accepted medical use.
Leonard Howell, a professor of psychiatry at Emory studying the pro-social effects of MDMA says that users should not equate “pure” with “safe.”
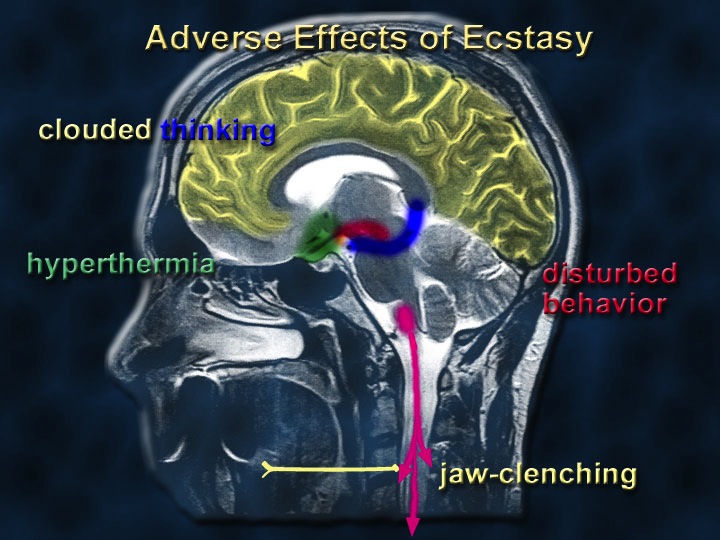
“Just because it’s pure doesn’t mean it’s safe. Pure MDMA has bad effects on its own right,” he says. The main problem is that MDMA causes core body temperatures to rise too high, and that holds true whether the drug is pure or not, he says.
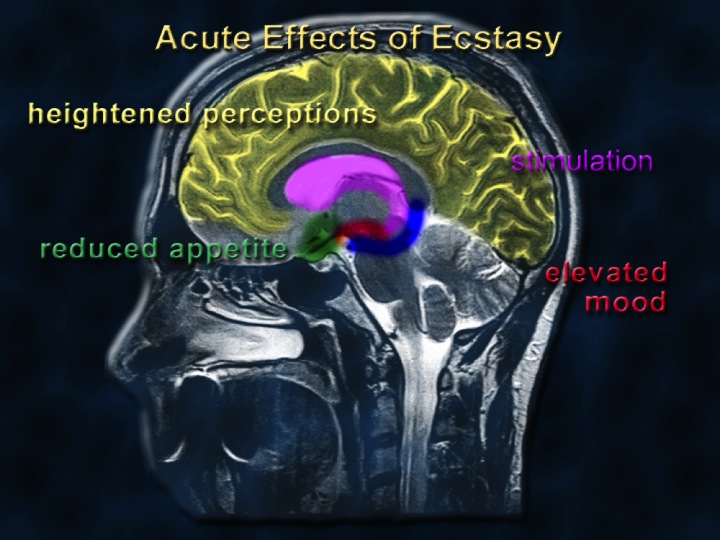
Howell explains that the pro-social effects of the drug, such as the feelings of empathy and human warmth make MDMA more popular at parties than many drugs such as mushrooms or LSD.
Images courtesy of National Institute on Drug AbuseImages courtesy of National Institute on Drug Abuse
The Drug Abuse Warning Network (DAWN) reports that the most MDMA users are between the ages of 18 and 20. DAWN also reported a 123 percent increase in MDMA-related hospital visits from 2004 to 2009.
Molly is prevalent at music festivals like Bonaroo and Electric Daisy Carnival, which are becoming more and more popular across the United States.
Although the drug first became popular among fans of electronic dance music about a decade ago, hip-hop artists have now recently adopted it as well. Molly has been referenced so many times in recent hip-hop songs that Complexmusic.com has started a “History of Rappers Referencing Molly in Songs” page. Most notably, Kanye West references it in his single “Mercy.”
Everyone seems to be talking about Molly these days, but nobody seems to be saying the same thing.
The one thing people do seem to agree on however is what it feels like when you’re “rolling.” “I didn’t care about anything but the music and the feeling of everything,” Sarah says. “I was all about the sensations. It was weird, but it was awesome.”
Another college senior, who requested anonymity, described it as “an incredible euphoric feeling that lasts for many hours.”
Molly comes in pill or powder form and can be gummed, inhaled, swallowed or parachuted—folded up into a tissue and swallowed. Users describe a bitter taste and often a tingly sensation in the mouth when the drug is ingested.
A typical dose is around .5 grams commonly taken in smaller doses over several hours according to users. When the euphoria begins to fade away users tend to take a bit more.
MDMA is a stimulant and that “awesome” euphoria is caused by a release of the neurotransmitters, norepinephrine, dopamine and serotonin, according to Howell.
Dr. Linda Grabbe, an assistant clinical psychiatric professor at Emory’s Nell Hodgson School of Nursing, says that the release of serotonin causes a release of the hormone oxytocin, commonly known as “the love hormone.” This is what causes the feelings of empathy and human warmth that make it so popular at parties, she says.
“What people say is it gives them a great sort of social connection with other people and released inhibitions,” she says.
The release of neurotransmitters, messengers of the brain cells, is followed by a subsequent depletion, often leaving users with feelings of depression that can be short or long term, Grabbe says.
Most formal institutions like The National Institute on Drug Abuse and the DEA do not distinguish between Molly and Ecstasy, making it impossible to know the exact number of users.
Law enforcement agencies have a similar issue distinguishing between the drugs, and because MDMA has no identifiable smell like alcohol or marijuana it is hard to detect once it is ingested. Neither the Emory Police Department nor Emory University Emergency Medical Services (EEMS) record any cases involving use of MDMA. Kevin Applegate, president of EEMS says they would diagnose someone on Molly with an “altered mental state,” the same description given to someone with alcohol poisoning or a concussion.
MDMA first hit the party scene in Ecstasy pills in the early 1990s, but rumors about its composition led users to Ecstasy’s more “pure” cousin Molly.
Sarah did not know the difference between Molly and Ecstasy when she first took the drug, but she and her friends looked up the symbol printed on their pills and found a website for a company claiming to have made the drug. She says she did not necessarily trust the website, but it made her feel better about trying Molly.
Both students purchased MDMA from a “friend of a friend.” Sarah bought pills for $10 each, but according to other users, Molly usually sells for around $7 to $10 per .1 grams—or around $30 a dose.
Howell says that if users are buying the drug illegally there is no way for them to know exactly what chemicals they are getting. He says that users who think the drug is pure MDMA are “just crazy.”
He says that most MDMA-related emergency room visits occur because of seizures, hyperthermia and dehydration. Because the drug is most often taken at parties or concerts, users often do not realize how tired and dehydrated they become after dancing and sweating continuously for hours he says.
Grabbe says many patients are hospitalized after combining MDMA with alcohol or other drugs. She says because MDMA affects temperature control in the body extreme cases result in hyperthermia, or overheating. Other side effects include electrolyte abnormalities, cardiac episodes and comas. She says many negative side effects occur when users combine drugs, or have a pre-existing condition that is aggravated by the MDMA.
Howell says there is a stigma against MDMA among scientists who study the drug because sustained use can lead to a neurotoxicity to serotonin, which means a long-term deficit of serotonin neurons in the brain. He says scientists have seen the effects of this deficit in sophisticated cognitive tests. The image below shows the depletion of serotonin in the brains of monkeys tested for the effects of MDMA.
He says it is difficult to convince young people about the long-term negative effects of MDMA use. “So they’re more living for the moment, and for the moment you know the drug appears to be safe,” he says.
Grabbe thinks that users are doing more research about drugs before they use them than in the past. “I think initially it was thought to be very safe, but now people are really understanding that there are health consequences so they’re beginning to get smarter about it,” she says.
She thinks peer education would be the most effective way to prevent use. “I’m an older nurse so me coming in and saying ‘you know, you really don’t want to go there,’ isn’t going to have a lot of impact necessarily,” she says.
Sarah might be just the peer to educate others. She is an example of MDMA use gone wrong.
In the hospital after losing feeling in her legs, she showed symptoms of hyponatremia, or sodium deficiency, which is common in MDMA users who drink too much water to avoid dehydration. While testing for hyponatremia, doctors discovered that she had an undiagnosed potassium deficiency, and after using MDMA she had almost no potassium left in her system. She spent the night in the hospital with an IV regaining control over the muscles in her legs.
Even though she knows her case is unique, she says it was enough to convince her never to do the drug again. “Its popularity has decreased with me,” she says.
She says she thinks what is most dangerous about Molly is its accessibility. “I definitely would think that it’s more dangerous because like when you’re at a party so many people have it and people tend to take more,” she says.
Sarah says Molly is not confined to electronic concerts anymore. Several friends of hers have taken the drug on a normal Saturday night out, she says.
The E.R. Crisis. What’s causing us to choose emergency medical care, and the steps we need to take before the crisis becomes a disaster.
Dale Davis has no college degree, no medical training, but could be considered an expert on the inner workings of a hospital emergency room. He suffers from cirrhosis of the liver, gout, and cognitive disabilities from a traumatic brain injury from a motorcycling accident. Due to this impressive list of ailments, he visits his local E.R. about three times a month, sometimes more. “There’s no comfort level at all in a big city hospital,” says Davis. “I know a lot about…metro hospitals where there is a lot of chaos in the emergency room, a lot of waiting.”
According to Davis’ experience, not everyone that comes to the E.R. is in critical condition. “Some of the people that are there, are there just for the sake of being there and aren’t really there for an emergency at all. And then some of the people there that are really there for emergencies, can suffer greatly.”
This chaos that Davis mentions, is the re-emerging and troubling trend that experts call “The E.R. Crisis.” The E.R. Crisis is a blanket phrase for the overcrowding of emergency rooms nationwide, especially in urban, densely populated places like Atlanta. The New England Journal of Medicine has published that visits to the E.R. have increased 26 percent since 2006. Why they are increasingly more crowded is a matter of opinion, and varies based on who you talk to. When it comes down to it, there are three possible answers; limited access to healthcare, diminished funds for hospital emergency care, or limited access to primary and preventive care options.
Dr. Stephen Pitts, doctor of Internal and Emergency Medicine at Grady Memorial Hospital, says lack of primary care physicians is a driving force of these mounting numbers. “People try to go to their doctor, but they can’t get in,” says Pitts. “To stay in business in primary care, you have to see another patient every fifteen minutes. If they can’t do that, they have to fire their office staff. Economic forces have put them in a bind, it makes them not able to give people the care they want to.” Dr. Pitts says that lack of access to primary care physicians is because of their unwillingness to accept uninsured patients and their preference for other private, more profit resulting insurance plans.
But it’s not the uninsured populations who are filling up E.R. beds. “The fact is the uninsured come to the E.R. less than other categories of patients. They’re worried about having a bill, and wait longer to be seen,” says Pitts. “Medicaid patients have the highest rate of visits, something like 50 to 60 people out of 100 in a year.”
In fact, with the Patient Protection and Affordable Care Act, the year 2014 is expected to cover 16 million more Americans with the Medicaid insurance plans. That is 16 million more people newly insured, and perhaps more likely to visit their local E.R. The projected data is troubling for most city hospitals. When the Medicaid expansion is implemented, the previously uninsured patients may no longer be concerned about the big bills, and may adopt the visiting frequencies of the patients who are currently on Medicaid.
The government is anxiously developing a solution to this impending aggravation of the E.R. Crisis. To stem the influx of emergency room patients, the government is developing programs to entice primary care physicians to be more likely to accept Medicaid insured patients. By offering more monetary incentives to take on these patients, the government hopes to lessen the burden of the emergency rooms, and channel patients to begin to choose primary and preventative avenues, rather than emergency care options.
Despite these measures, the initial stages may still be devastating. To some experts, the problem is the cost burden of E.R. visits and the toll it takes on the entire system.
Michael Rovinsky, President of Integrity Consulting Group, a healthcare consulting group based in Atlanta, says the E.R. is the currently the most expensive endeavor of the entire healthcare system and will continue to be.
The E.R. is the biggest problem in healthcare, says Rovinsky. “It is overused by people who do not have a critical condition. The worst part of emergency care, is it’s the most expensive kind of healthcare. It costs the payers of healthcare a tremendous amount of money.” According to Rovinsky, the behavior, and the culture of the population who uses the E.R. as a primary care solution, will be among the hardest thing to change.
Likewise, many lawmakers are not in favor of the law, and will further hinder primary care expansion to prevent extreme overcrowding in emergency departments. Rovinsky says, this will only worsen the current problems. “A number of governors across the country are against the expansion of Medicaid. Hospitals treat patients anyway, without any money. It’s in their best interest to accept the expansions, because it’s costing the system more money without it. The ultimate goal is the overall reduction of healthcare costs for the entire population.”
More importantly, there is an underlying issue that is often neglected and failed to be targeted in government acts or motions of reform. Patient responsibility is also a topic this rarely mentioned. If everyone was insured, everyone had a primary care physician, and everyone had access to these programs, people still will continue to get acutely ill.
Rovinsky says, it’s because of an unwillingness of some patients to take care of themselves. He explains it simply that the biggest cost to healthcare is using healthcare services. Things that prevent acute illness lessen the amount of money being spent. Simply stated, yet rarely understood, or even mentioned in public debate.
“Anything that leads to poor health, tremendously increases the cost of healthcare,” says Rovinsky. “The big thing that no one will speak about is personal responsibility for wellness. The obesity crisis, the diabetes crisis, drives the cost of healthcare up. The public should take personal responsibility for living a healthier lifestyle. That’s the missing piece in the healthcare discussion.”
All in all, even if all these reforms and preventive measures take a successful hold, the healthcare world is just a world of maybes. Maybe people will seek primary care physicians instead of the emergency room. Maybe primary care physicians will take to the incentives to take on Medicaid patients.
Maybe, maybe not.
In the meantime, the crisis will rage on. Until 2014, it is very unlikely experts will have a clear vision of the new horizons of healthcare. People like Dale Davis will continue to be subject to an increasingly burdened system, with a very foggy future.
But he remains optimistic about the quality of care he receives. “I’ve been extremely lucky,” says Davis. “I’ve been uninsured through times of my life, and I haven’t always been fortunate enough to get the care I needed. But it comes down to taking care of yourself too. You stop drinking, you stop treating your body badly, and you can save yourself a lot.”
With eagerness in his voice, he looks forward to his placement on the transplant list for a new liver later this month. Davis also acknowledges the importance of personal responsibility in healthcare, and claims it’s what turned his life around.
“Yeah, it comes down to you. How badly you want the second chance. You have to prove you want to be healthy, you need to prove you deserve the new life. There’s always someone around the corner who may need it more than you, and that may be the one thing that will scare you straight.”
What with the classic red barstools and friendly Southern staff, the Majestic Diner at Poncey-Highland is very sweet. Many customers are regulars, there for the “homey feel,” of a place that has been serving “food that pleases” since 1929. Unquestionably, the atmosphere is nice.However, should we really be support a place that essentially sells future diabetes and heart attacks?
True to tradition, Majestic Diner offers heaping mounds of comfort food, an expression I’ve never quite understood. I don’t particularly feel comfortable when food upsets my digestive enzymes and halts the chance of nutrient uptake. Pancakes and syrup may feel wonderful in your belly for about five minutes, but shortly after peaking on the high glycemic index chart they skyrocket you down to the “I feel horrible” stage.
As soon as sugar enters the bloodstream, a rush of insulin and serotonin overtake your body, according to Dr. Gillian McKeith, author of You Are What You Eat. The sudden rise in sugar levels causes the insulin to break it down very quickly, causing a drop in both sugar and endorphins—ultimately making you feel worse.
Junk food is called junk for a reason. A hamburger is part of the fatty food group that clogs arteries, depletes calcium levels, and compromises the function of the heart. Pancakes and syrup are sweets, which cause severe blood sugar imbalances and mood swings. Sweets also disrupt the function of the spleen, liver, pancreas and intestines. Adding a milkshake? According to the National Institute of Health, 30 million of you probably can’t digest milk.
The diner did offer salads, but they were covered with pepperoni and ham. I’m not entirely certain there were vegetables under the thick blue cheese dressing.
Recent nutritional research is producing more and more evidence that sugar is addicting, so pretty much all processed food is addicting. In addition, Nature Neuroscience found that excess food intake can trigger alterations in the brain, creating a neurochemical dependency. The National Institute on Drug Abuse is finding an “overlap between drugs in the brain and food in the brain.” Brain scans demonstrated disturbances in the reward circuit of the brains of obese people and compulsive eaters, just like drug abusers.
That’s enough information to make me want to steer clear of this tradition of American existence.
I’m fine with the décor of the 1950s, but it’s time for an upgraded menu. Sorry Majestic Diner, your food just isn’t pleasing.
Majestic Diner
1031 Ponce De Leon Avenue NE, Atlanta, GA 30306 majesticdiner.com/