
Clinical question / background:
- Is there a simple clinical model to rule out pulmonary embolism in patients presenting to the emergency department?
Design:
- Prospective cohort study
- 930 participants in 4 Canadian Centers
- Inclusion: Adults with suspected PE with sxs < 30 days; chest pain or shortness of breath acute in onset
- Exclusion: UE DVT as likely source of PE, no sxs within 3 days of presentation, expected survival < 3 months, anticoagulation therapy for 24 hours or more, contraindication to contrast, pregnancy, < 18 y/o, unable to follow-up
Intervention:
- Implementation of clinical model to determine probability of PE
- 3 points – Clinical Signs/Sxs of DVT
- Objectively measured leg swelling and/or pain with palpation of deep veins
- 1.5 points – Tachycardia (HR> 100)
- 1.5 points – bed rest (except going to bathroom) for 72 hours, or surgery within previous 4 weeks
- 1.5 points – prior dx of DVT or PE
- 1 point – hemoptysis
- 1 point – malignancy (current rx, palliative care, or treatment within the preceding 6 months)
- 3 points – PE as most likely or as likely as alternative diagnosis based on physical exam and basic workup (EKG, CXR, screening labs)
- 3 points – Clinical Signs/Sxs of DVT
- Pretest Probability of PE based on Score
- < 2.0 points – low risk
- 2.0 – 6.0 points – moderate risk
- >6.0 points – high risk
- Primary Outcome
- 3-month occurrence of PE based on initial risk stratification
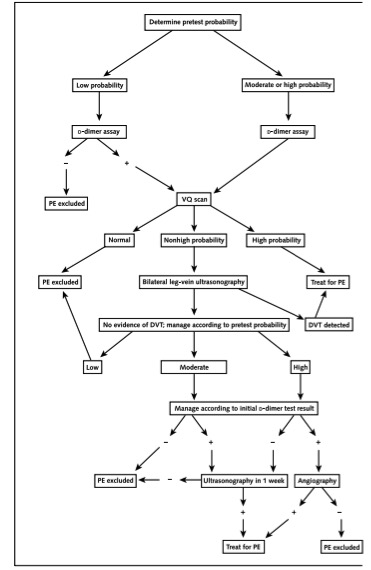
- Algorithm (see below)
Results:
- LOW pre-test probability – PE diagnosed in 1.3% at 3-month f/u
- MODERATE pre-test probability – PE diagnosed in 16.2% at 3-month f/u
- HIGH pre-test probability – PE diagnosed in 37.5% at 3-month f/u
Take-home:
- The Wells’ Criteria risk stratifies patients for pulmonary embolism (PE) and provides an estimated pre-test probability. The physician can then chose what further testing is required for diagnosing pulmonary embolism (I.E. d-dimer or CT angiogram or V/Q
Strengths:
- Simple to use; clear cut-offs
- Validated multiple times in multiple settings since original paper
Weaknesses / Critiques
- Subjective component of PE being most likely diagnosis can push score to intermediate range and lead to unnecessary testing
- Reliance on d-dimer for decision-making
Follow-up / Real World Application
- If patient determined to be low Risk, consider d-dimer testing
- Also in low-risk patients, can be used with the PERC as rule-out for PE
- The PERC rule can be applied to patients where the diagnosis of PE is being considered, but the patient is deemed low-risk. A patient deemed low-risk by physician’s gestalt who is also <50 years of age, with a pulse <100 bpm, SaO2≥ 95%, no hemoptysis, no estrogen use, no history of surgery/trauma within 4 weeks, no prior PE/DVT and no present signs of DVT can be safely ruled out and does not require further workup
- In medium / high risk patients, consider CTA (+/- d-dimer) or V/Q
- Calculator links
- http://www.mdcalc.com/wells-criteria-for-pulmonary-embolism-pe/
- http://www.mdcalc.com/perc-rule-for-pulmonary-embolism/