
Lit of the Week – 3/01/16
Clinical question / background:
- Can decision rules based on history and simple physical exam findings guide the use of radiography in acute ankle and foot injuries?
Design:
- Prospective study of 1032 patients with acute ankle injuries refining old ankle rules followed by validation in 453 patients
- 2 urban academic center emergency departments
- Inclusion: Adults (> 18 y/o) presenting after acute blunt ankle trauma
- Exclusion: Pregnant patients, children, injury > 10 days old, OSH transfers, patients returning for reassessment of same injury
- Patient evaluated by one of 21 study physicians according to pre-determined decision rules (details below)
- Primary outcome: detection of clinically significant fracture which is defined as fracture or avulsion > 3 cm
- Secondary outcomes: interobserver reliability
Intervention of Ankle and Foot Rules
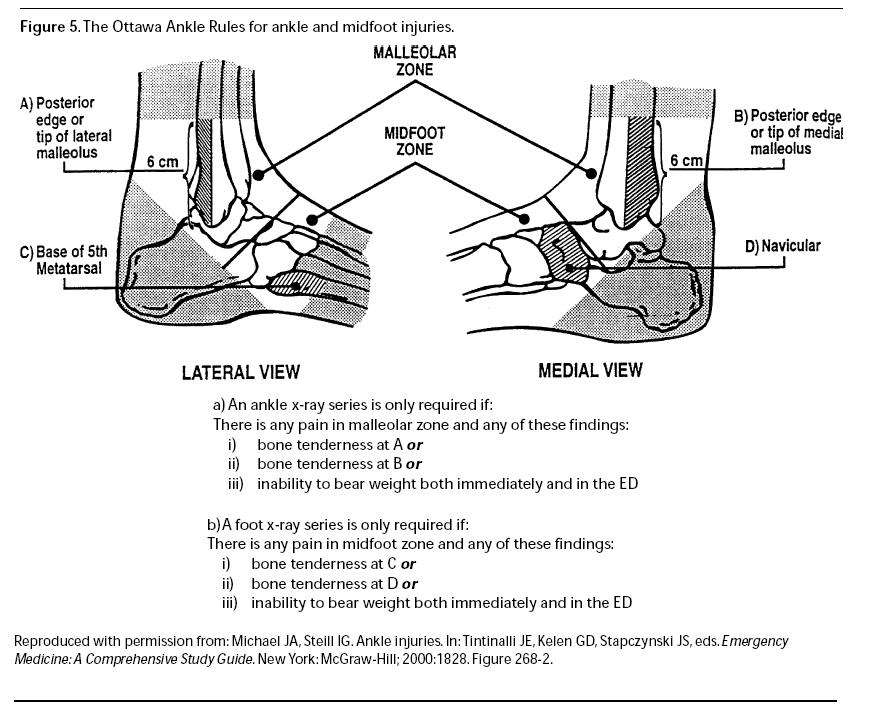
- Ankle Rules – ankle x-ray indicated for following physical findings
- Bony tenderness along posterior edge or tip of distal 6 cm of lateral malleolus
- Bony tenderness along posterior edge or tip of distal 6 cm of medial malleolus
- Inability to bear weight on injured extremity both immediately after injury or in the emergency department (four steps)
- Limping counts as bearing weight
- Foot Rules – foot x-ray indicated for following physical findings
- Bony tenderness at the navicular (medial aspect of foot)
- Bony tenderness at the base of the 5th metatarsal
- Inability to bear weight on injured extremity both immediately after injury or in the emergency department (four steps)
- Limping counts as bearing weight
Results:
- Ankle Rules
- Sensitivity 100%, Specificity 39% in refinement cohort
- Sensitivity 100%, Specificity 49% in validation cohort
- Foot Rules
- Sensitivity 98%, Specificity 70% in refinement cohort
- Sensitivity 100%, Specificity 79% in validation cohort
Take-home:
- If ankle pain is present and there is tenderness over the posterior 6 cm or tip of the posterior or lateral malleolus, then an ankle-ray is indicated
- If midfoot pain is present and there is tenderness over the navicular or the base of the fifth metatarsal, then a foot-xray is present
- If there is ankle or midfoot pain and the patient is unable to take four steps both immediately and in the emergency department, then x-ray of the painful area is indicated
- In patients that fail to fulfill the above rules, radiography likely not indicated but defer to clinical judgment
Strengths:
- Well-designed, large study
- High kappa values indicating interobserver reliability
- e. multiple examining physicians likely to get similar exam results on patients and implement rules appropriately
- can reduce # of x-rays and speed up patient turnover in ER
Weaknesses / Critiques
- poor specificity in the ankle cohort, relatively weak specificity in foot cohort
- not useful for calcaneal injuries, distal foot injuries
- careful with patients who are intoxicated, uncooperative, have painful or distracting injuries, or diminished neurologic function in extremity that can limit usefulness of exam